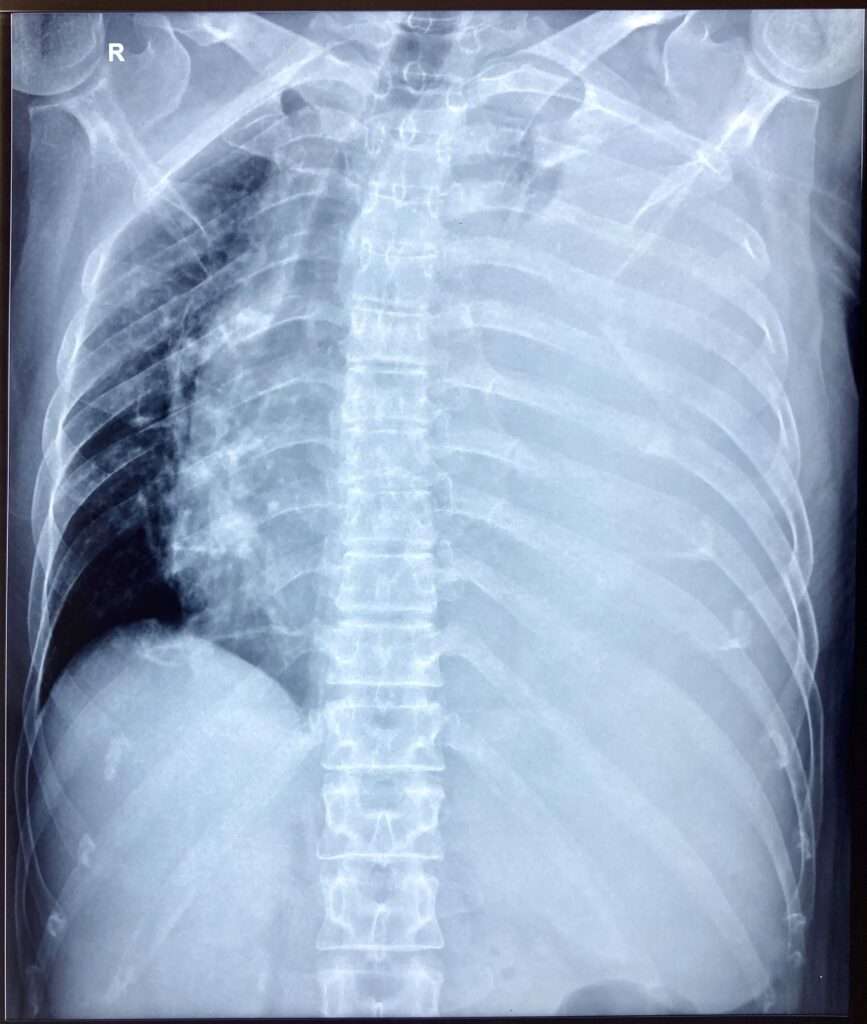
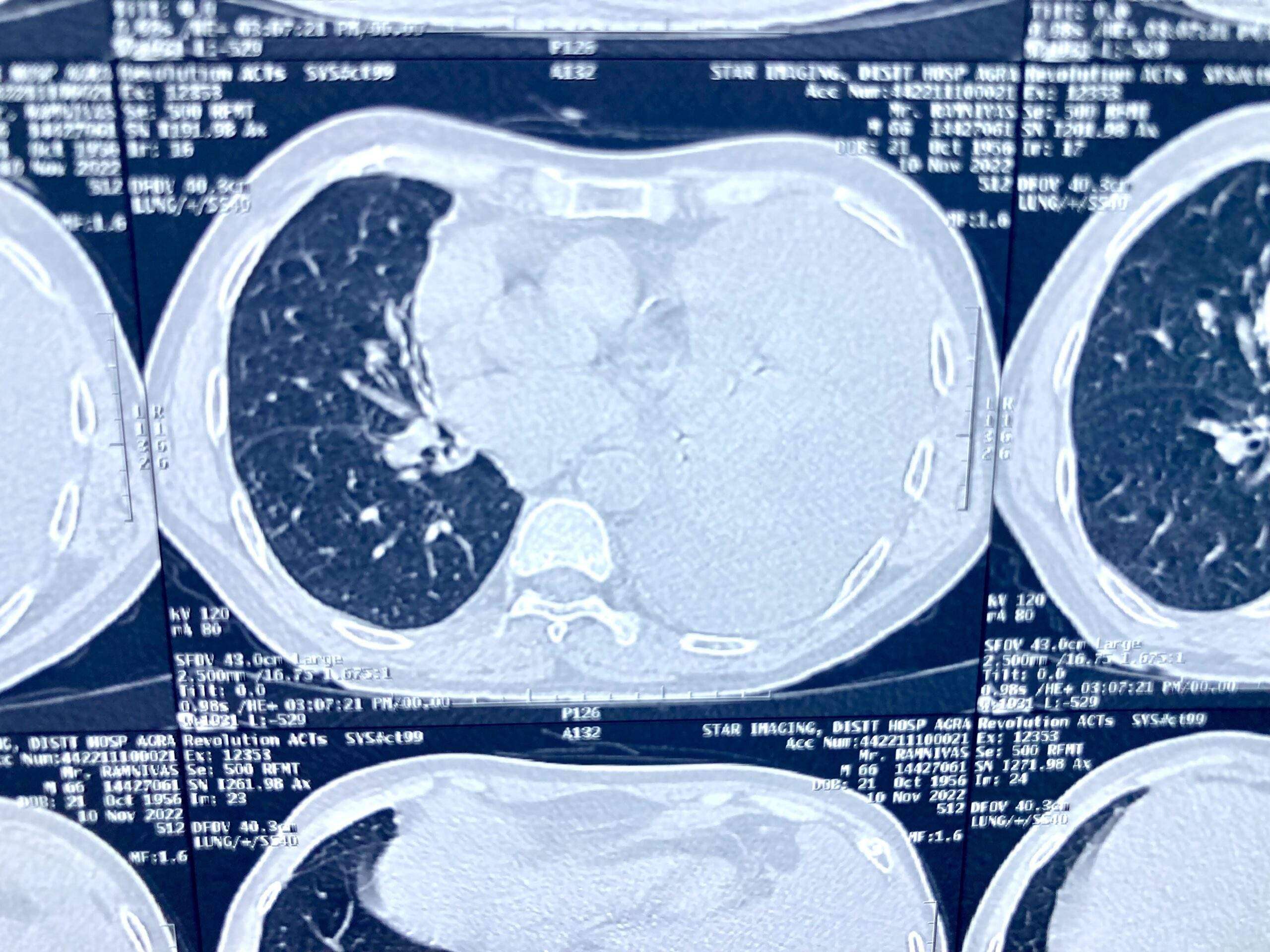
Pleural effusion, sometimes referred to as “water on the lungs,” is the build-up of excess fluid between the layers of the pleura outside the lungs. The pleura are thin membranes that line the lungs and the inside of the chest cavity and act to lubricate and facilitate breathing. Normally, a small amount of fluid is present in the pleura.
Pleural effusionPleural Effusion Aspiration Site
Symptoms
Some patients with pleural effusion have no symptoms, with the condition discovered on a chest X-ray that is performed for another reason. The patient may have unrelated symptoms due to the disease or condition that has caused the effusion. Symptoms of pleural effusion include:
Chest pain
Dry, non-productive cough
Dyspnea (shortness of breath, or difficult, labored breathing)
Orthopnea (the inability to breathe easily unless the person is sitting up straight or standing erect)
Causes
The most common causes of transudative (watery fluid) pleural effusions include:
Heart Failure
Pulmonary Embolism
Cirrhosis
Post open heart surgery
Exudative (protein-rich fluid) pleural effusions are most commonly caused by:
Pneumonia including Tuberculosis
Cancer
Pulmonary Embolism
Kidney Disease
Inflammatory disease
Other less common causes of pleural effusion include:
Autoimmune disease
Bleeding (due to chest trauma)
Chylothorax (due to trauma)
Rare chest and abdominal infections
Asbestosis pleural effusion (due to exposure to asbestos)
Meig’s syndrome (due to a benign ovarian tumor)
Ovarian hyperstimulation syndrome
Certain medications, abdominal surgery and radiation therapy may also cause it. It may occur with several types of cancer including lung cancer, breast cancer and lymphoma. In some cases, the fluid itself may be malignant (cancerous), or may be a direct result of chemotherapy.
Diagnosis
The tests most commonly used to diagnose and evaluate include:
Chest X-ray
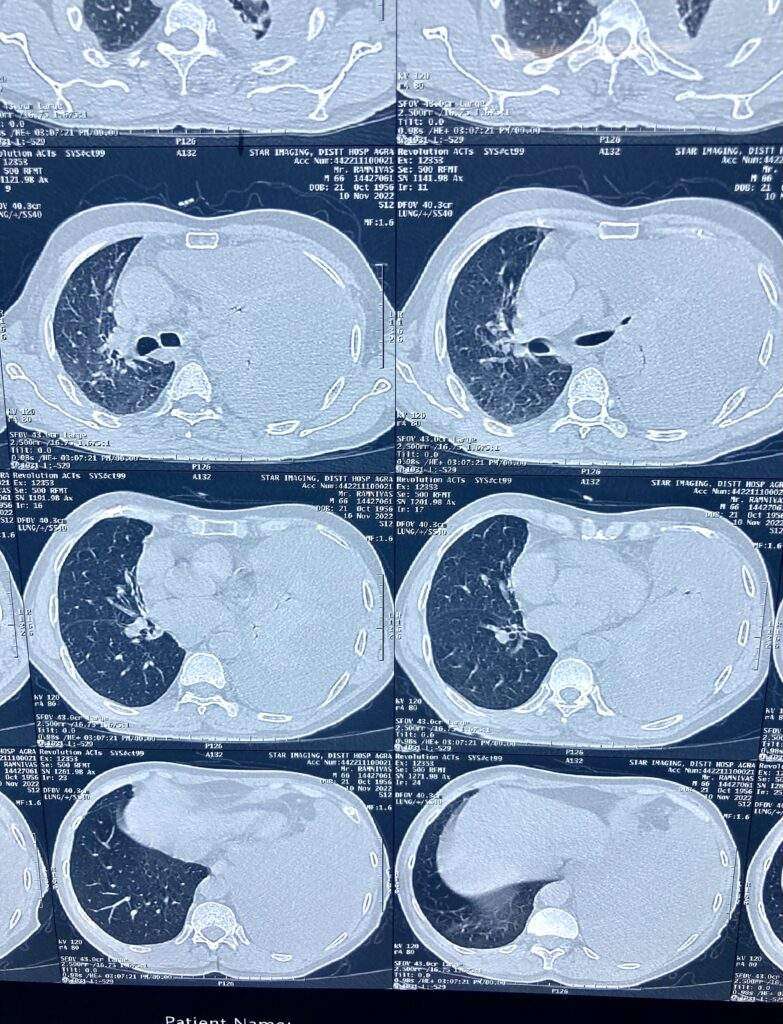
Computed Tomography (CT) of the chest
Ultrasonography of the chest
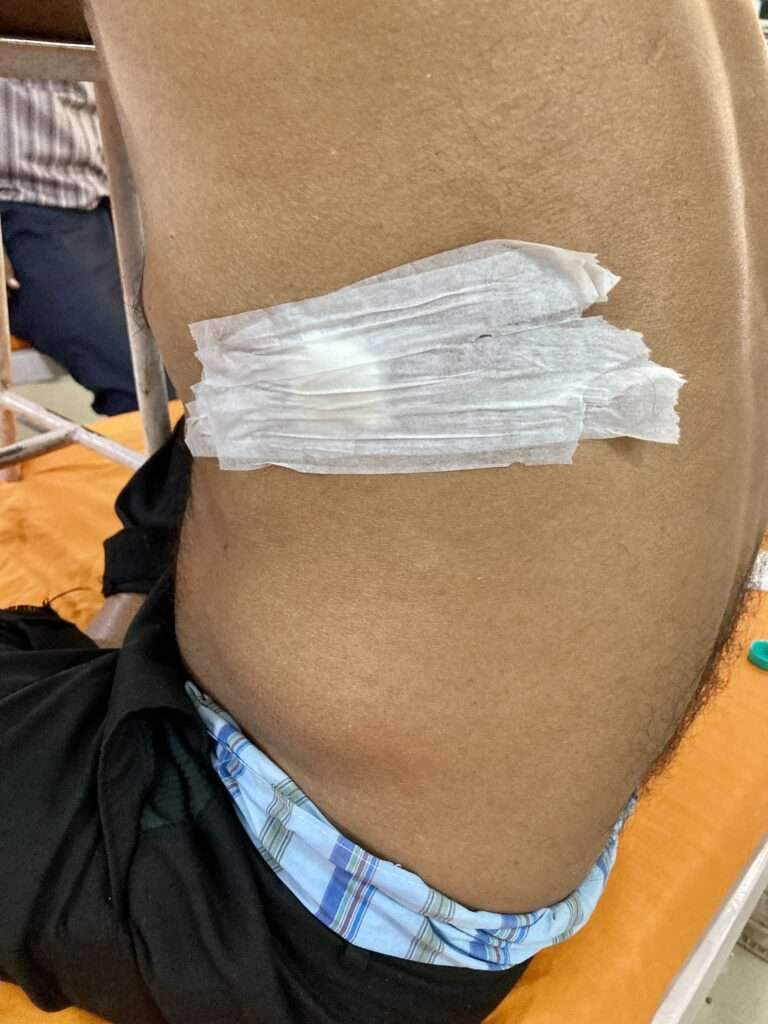
Thoracentesis (a needle is inserted between the ribs to remove a biopsy, or sample of fluid)
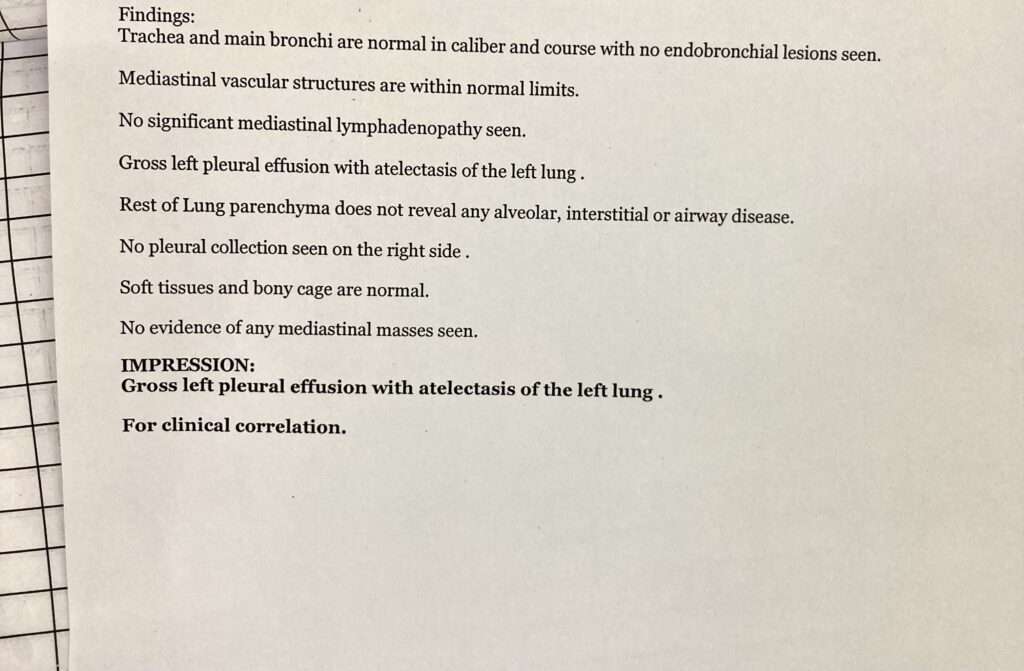
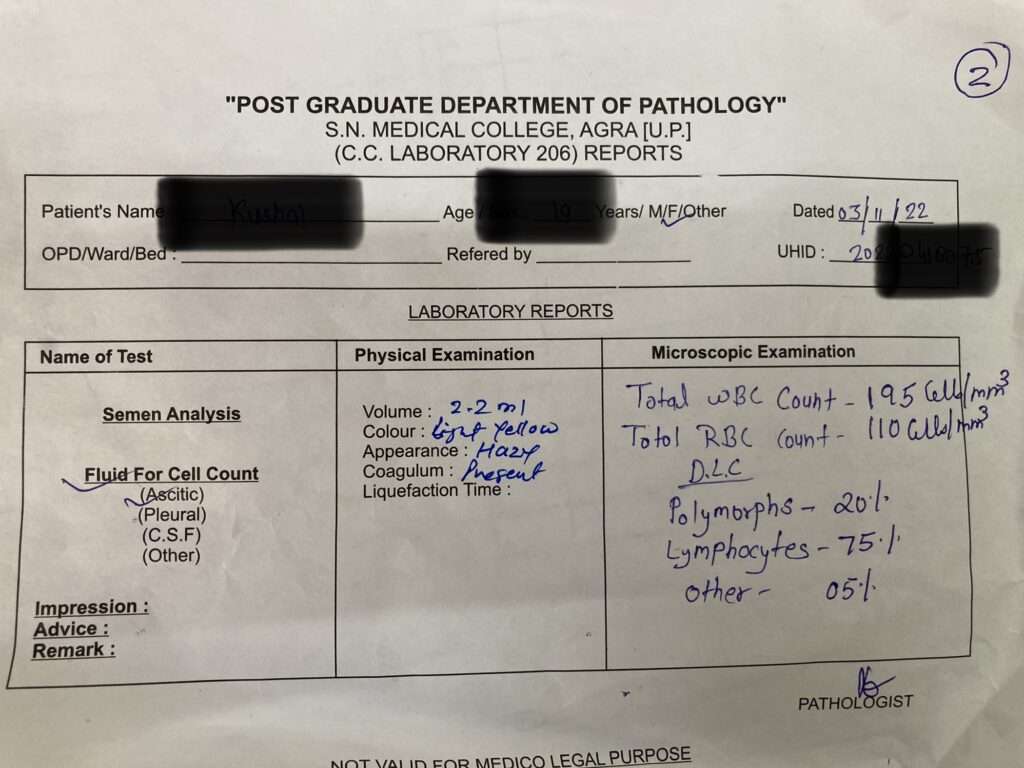
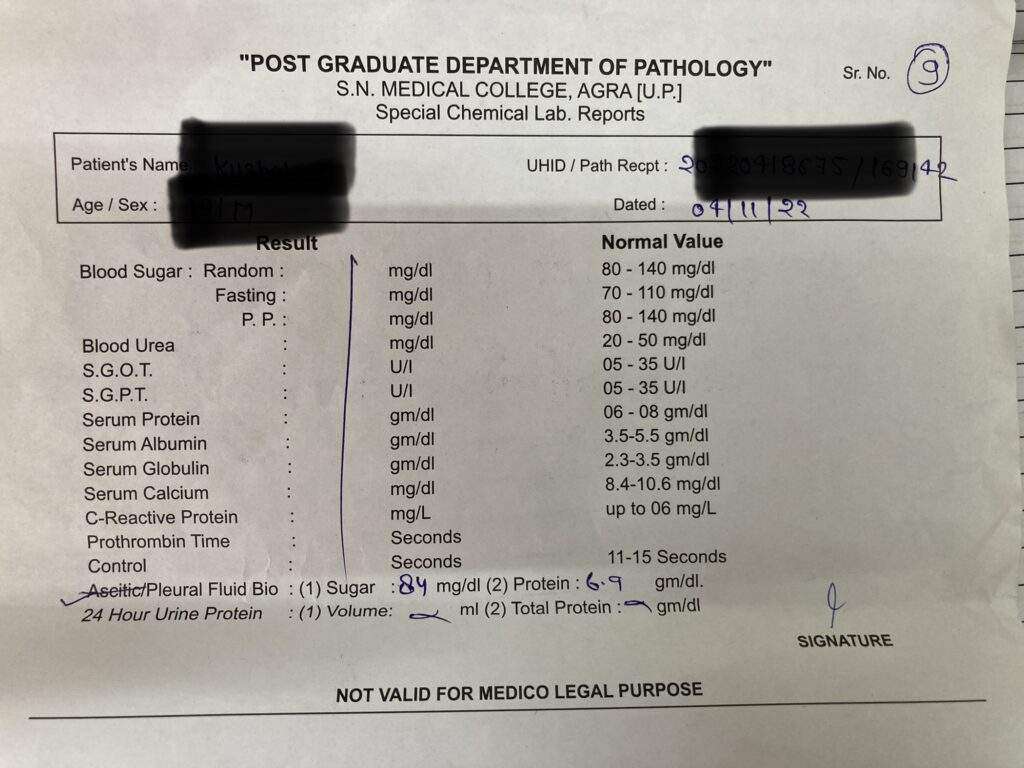
Pleural fluid analysis (an examination of the fluid removed from the pleura space)
Left Sided Massive Pleural Effusion with Mediastinal ShiftingPleural Effusion Fluid Aspiration (Diagnostic)
When it has remained undiagnosed despite previous, less-invasive tests, thoracoscopy may be performed. Thoracoscopy is a minimally invasive technique, also known as video-assisted thoracoscopic surgery, or VATS, performed under general anesthesia that allows for a visual evaluation of the pleura). Often, treatment of the effusion is combined with diagnosis in these cases.
Treatment
Treatment is based on the underlying condition and whether the effusion is causing severe respiratory symptoms, such as shortness of breath or difficulty breathing.
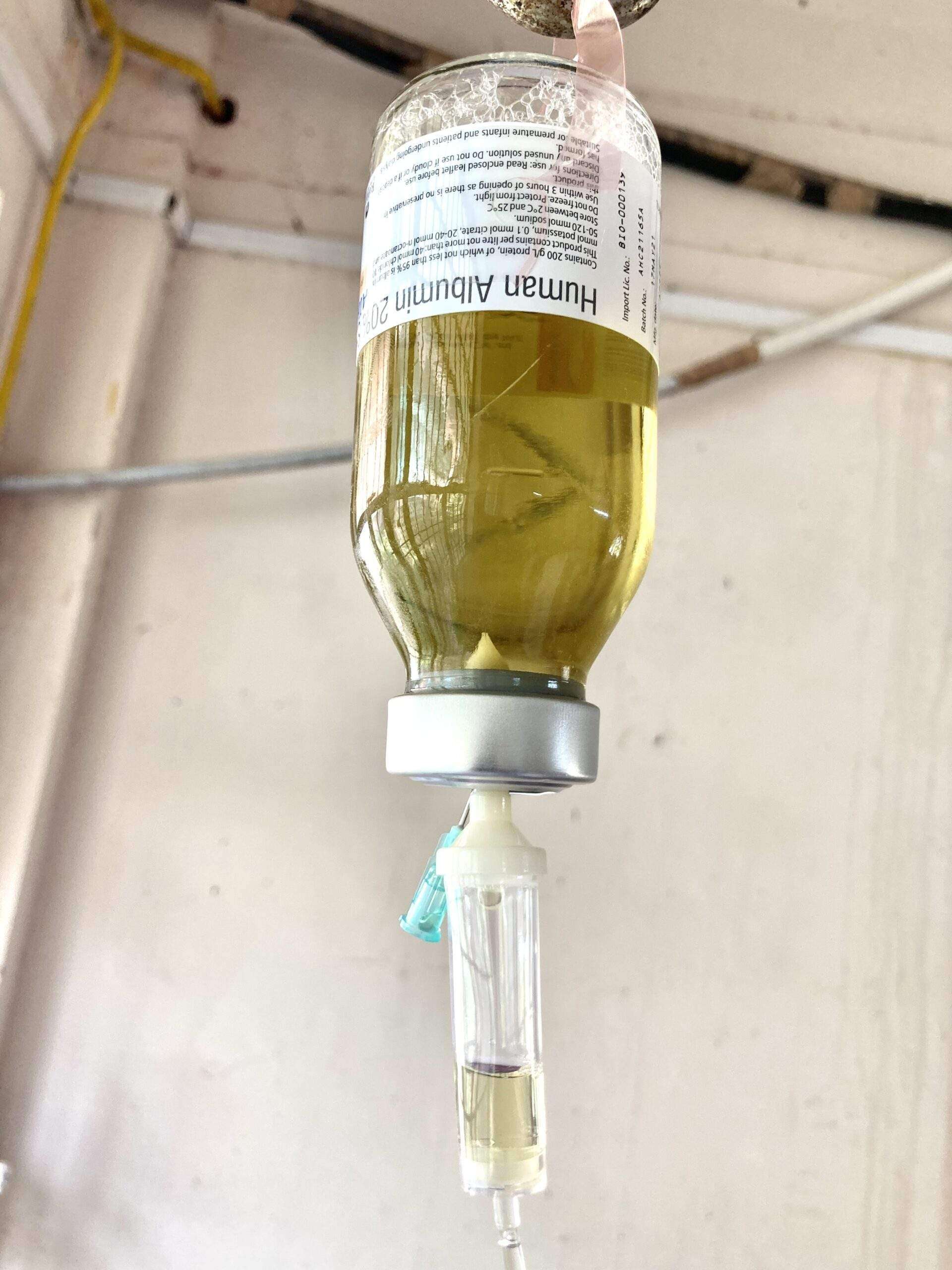
Diuretics and other heart failure medications are used to treat pleural effusion caused by congestive heart failure or other medical causes. A malignant effusion may also require treatment with chemotherapy, radiation therapy or a medication infusion within the chest.
A pleural effusion that is causing respiratory symptoms may be drained using therapeutic thoracentesis or through a chest tube (called tube thoracostomy).
For patients who that are uncontrollable or recur due to a malignancy despite drainage, a sclerosing agent (a type of drug that deliberately induces scarring) occasionally may be instilled into the pleural cavity through a tube thoracostomy to create a fibrosis (excessive fibrous tissue) of the pleura (pleural sclerosis).
Pleural sclerosis performed with sclerosing agents (such as talc, doxycycline, and tetracycline) is 50 percent successful in preventing the recurrence of pleural effusions.
Surgery
If cannot be managed through drainage or pleural sclerosis may require surgical treatment.
The two types of surgery include:
Video-assisted thoracoscopic surgery (VATS)
A minimally-invasive approach that is completed through 1 to 3 small (approximately ½ -inch) incisions in the chest. Also known as thoracoscopic surgery, this procedure is effective in managing pleural effusions that are difficult to drain or recur due to malignancy. Sterile talc or an antibiotic may be inserted at the time of surgery to prevent the recurrence of fluid build-up.
Thoracotomy (Also referred to as traditional, “open” thoracic surgery)
A thoracotomy is performed through a 6- to 8-inch incision in the chest and is recommended for pleural effusions when infection is present. A thoracotomy is performed to remove all of the fibrous tissue and aids in evacuating the infection from the pleural space. Patients will require chest tubes for 2 days to 2 weeks after surgery to continue draining fluid.
Surgeon will carefully evaluate you to determine the safest treatment option and will discuss the possible risks and benefits of each treatment option.
Ascites is a condition in which fluid collects in spaces within your abdomen. If severe, ascites may be painful. The problem may keep you from moving around comfortably. Ascites can set the stage for an infection in your abdomen. Fluid may also move into your chest and surround your lungs. This makes it hard to breathe.
Indications for Ascitic Fluid Tap (Abdominal Paracentesis)
To aid diagnosis of the cause of ascites or in the diagnosis or exclusion of SBP
A diagnostic paracentesis should be performed in all patients with new onset grade 2 or 3 ascites, and in all patients hospitalized for worsening of ascites or any complication of cirrhosis
Urinary incontinence — the loss of bladder control — is a common and often embarrassing problem. The severity ranges from occasionally leaking urine when you cough or sneeze to having an urge to urinate that’s so sudden and strong you don’t get to a toilet in time.
It is not just a medical problem. It can affect emotional, psychological and social life. Many people who have urinary incontinence are afraid to do normal daily activities. They don’t want to be too far away from toilet. It can keep people away from enjoying life.
Though it occurs more often as people get older, urinary incontinence isn’t an inevitable consequence of aging. If urinary incontinence affects your daily activities, don’t hesitate to see your doctor. For most people, simple lifestyle and dietary changes or medical care can treat symptoms of urinary incontinence.
Our urinary system is made up of the kidneys, ureters, bladder and urethra. These parts do several functions. They filter, store and remove waste from your body. Kidneys are the filters of your body. Waste products are removed from your blood by the kidneys, creating urine. The urine then moves down through two thin tubes called the ureters. The ureters connect to the bladder, where the urine will collect until it’s time to leave the body.
Urinary bladder is like a storage tank — once the bladder is full, the brain sends a signal that it’s time to urinate. Urine then leaves the bladder when a muscle opens up (sphincter), allowing the urine to flow freely out of the body through the urethra.
When this system is working smoothly, we usually have time to get to a bathroom before needing to urinate and we don’t experience any leakage of urine. Urinary incontinence can happen when these parts don’t operate as they should. This can happen for many different reasons throughout your life.
Many people think that incontinence is a normal part of aging that can’t be helped. While it is true that your risk of incontinence increases as we get older, there are also treatments available to help you manage this condition. Incontinence doesn’t have to disrupt your life and keep you from being active.
Symptoms
Many people experience occasional, minor leaks of urine. Others may lose small to moderate amounts of urine more frequently.
5 Types of urinary incontinence include:
Stress incontinence. Urine leaks when you exert pressure on your bladder by coughing, sneezing, laughing, exercising or lifting something heavy.
Urge incontinence. You have a sudden, intense urge (feel) to urinate followed by an involuntary loss of urine. You may need to urinate often, including throughout the night. Urge incontinence may be caused by a minor condition, such as infection, or a more severe condition such as a neurological disorder or diabetes.
Overflow incontinence. You experience frequent or constant dribbling of urine due to a bladder that doesn’t empty completely.
Functional incontinence. A physical or mental impairment keeps you from making it to the toilet in time. For example, if you have severe arthritis, you may not be able to unbutton your pants quickly enough.
Mixed incontinence. You experience more than one type of urinary incontinence — most often this refers to a combination of stress incontinence and urge incontinence.
Causes
Urinary incontinence can be caused by everyday habits, underlying medical conditions or physical problems. A thorough evaluation by your doctor can help determine what’s behind your incontinence.
Temporary urinary incontinence
Certain drinks, foods and medications may act as diuretics — stimulating your bladder and increasing your volume of urine. They include:
Alcohol
Caffeine
Carbonated drinks and sparkling water
Artificial sweeteners
Chocolate
Chili peppers
Foods that are high in spice, sugar or acid, especially citrus fruits
Heart and blood pressure medications, sedatives, and muscle relaxants
Large doses of vitamin C
Urinary incontinence may also be caused by an easily treatable medical condition, such as:
Urinary tract infection. Infections can irritate your bladder, causing you to have strong urges to urinate and, sometimes, incontinence.
Constipation. The rectum is located near the bladder and shares many of the same nerves. Hard, compacted stool in your rectum causes these nerves to be overactive and increase urinary frequency.
Persistent urinary incontinence
Urinary incontinence can also be a persistent condition caused by underlying physical problems or changes, including:
Pregnancy. Hormonal changes and the increased weight of the fetus can lead to stress incontinence.
Childbirth. Vaginal delivery can weaken muscles needed for bladder control and damage bladder nerves and supportive tissue, leading to a dropped (prolapsed) pelvic floor. With prolapse, the bladder, uterus, rectum or small intestine can get pushed down from the usual position and protrude into the vagina. Such protrusions may be associated with incontinence.
Changes with age. Aging of the bladder muscle can decrease the bladder’s capacity to store urine. Also, involuntary bladder contractions become more frequent as you get older.
Menopause. After menopause, women produce less estrogen, a hormone that helps keep the lining of the bladder and urethra healthy. Deterioration of these tissues can aggravate incontinence.
Enlarged prostate. Especially in older men, incontinence often stems from enlargement of the prostate gland, a condition known as benign prostatic hyperplasia.
Prostate cancer. In men, stress incontinence or urge incontinence can be associated with untreated prostate cancer. But more often, incontinence is a side effect of treatments for prostate cancer.
Obstruction. A tumor anywhere along your urinary tract can block the normal flow of urine, leading to overflow incontinence. Urinary stones — hard, stone like masses that form in the bladder — sometimes cause urine leakage.
Neurological disorders. Multiple sclerosis, Parkinson’s disease, a stroke, a brain tumor or a spinal injury can interfere with nerve signals involved in bladder control, causing urinary incontinence.
Risk Factors
Factors that increase your risk of developing urinary incontinence include:
Gender. Women are more likely to have stress incontinence. Pregnancy, childbirth, menopause and normal female anatomy account for this difference. However, men who have prostate gland problems are at increased risk of urge and overflow incontinence.
Age. As you get older, the muscles in your bladder and urethra lose some of their strength. Changes with age reduce how much your bladder can hold and increase the chances of involuntary urine release.
Being overweight. Extra weight increases pressure on your bladder and surrounding muscles, which weakens them and allows urine to leak out when you cough or sneeze.
Smoking. Tobacco use may increase your risk of urinary incontinence.
Family history. If a close family member has urinary incontinence, especially urge incontinence, your risk of developing the condition is higher.
Some diseases. Neurological disease or diabetes may increase your risk of incontinence.
Diagnosis
Your doctor is likely to start with a thorough history and physical exam. You may then be asked to do a simple maneuver that can demonstrate incontinence, such as coughing.
Urinalysis. A sample of your urine is checked for signs of infection, traces of blood or other abnormalities.
Bladder diary. For several days you record how much you drink, when you urinate, the amount of urine you produce, whether you had an urge to urinate and the number of incontinence episodes.
Postvoid residual measurement. You’re asked to urinate (void) into a container that measures urine output. Then your doctor checks the amount of leftover urine in your bladder using a catheter or ultrasound test. A large amount of leftover urine in your bladder may mean that you have an obstruction in your urinary tract or a problem with your bladder nerves or muscles.
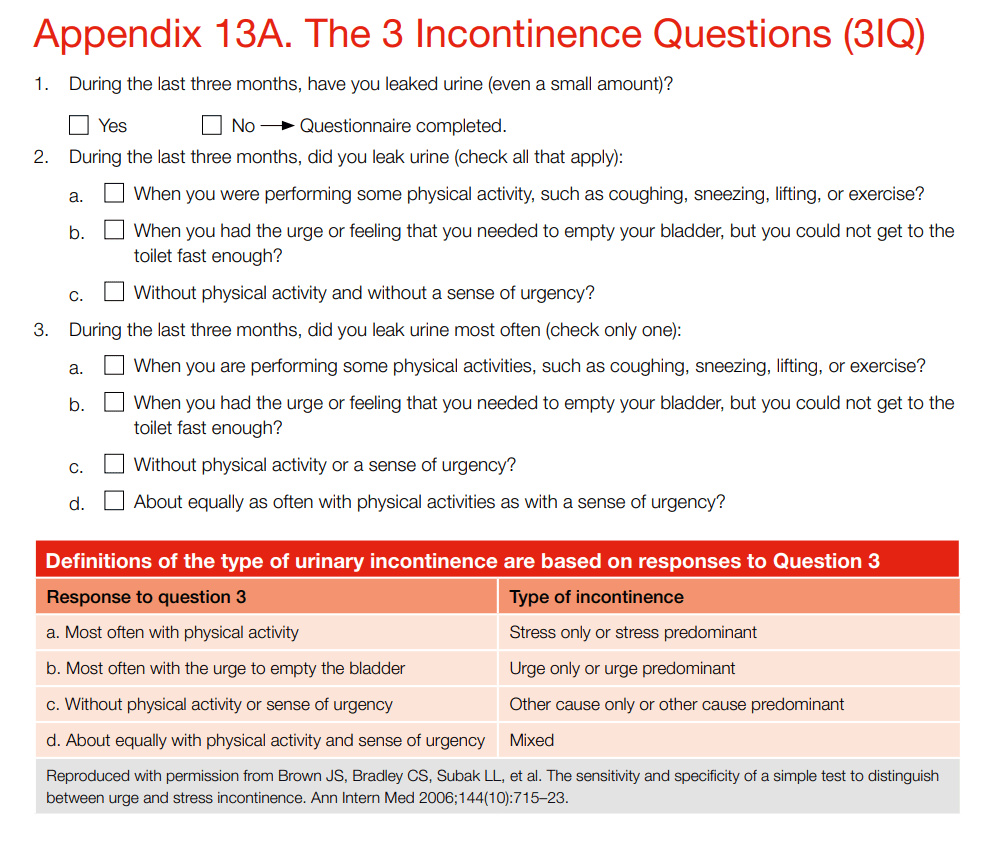
3IQ (Incontinence Questionnaire)
These questions are differentiate between these types of incontinence.
3IQ (Incontinence Questionnaire)
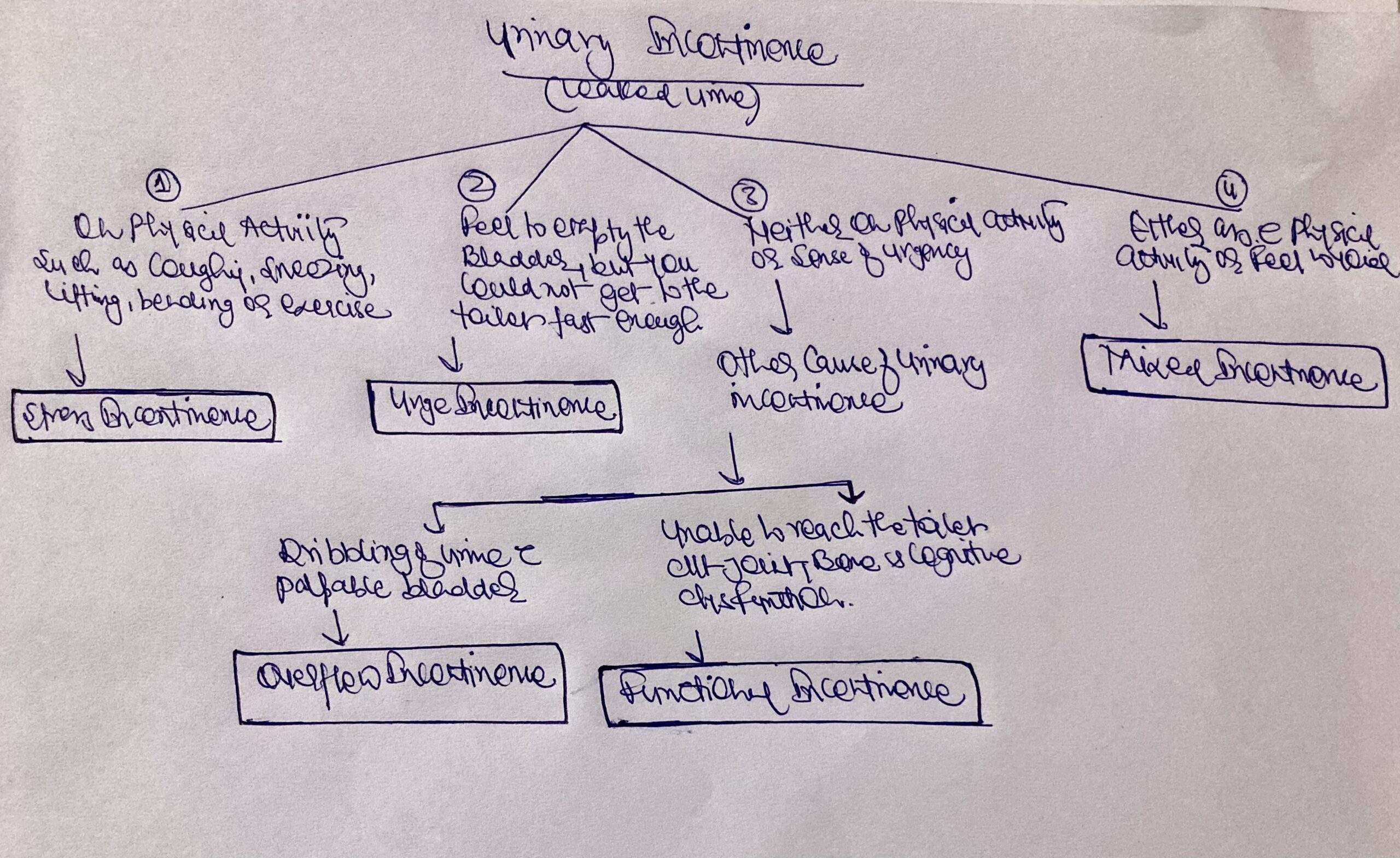
Urinary Incontinence Algorithm
urinary incontinence algorithm
Treatment
Behavioral techniques
Bladder training, to delay urination after you get the urge to go. You may start by trying to hold off for 10 minutes every time you feel an urge to urinate. The goal is to lengthen the time between trips to the toilet until you’re urinating only every 2.5 to 3.5 hours.
Double voiding, to help you learn to empty your bladder more completely to avoid overflow incontinence. Double voiding means urinating, then waiting a few minutes and trying again.
Scheduled toilet trips, to urinate every two to four hours rather than waiting for the need to go.
Fluid and diet management, to regain control of your bladder. You may need to cut back on or avoid alcohol, caffeine or acidic foods. Reducing liquid consumption, losing weight or increasing physical activity also can ease the problem.
Pelvic Floor Muscles Exercises
Also known as Kegel exercises, these techniques are especially effective for stress incontinence but may also help urge incontinence.
To do pelvic floor muscle exercises, imagine that you’re trying to stop your urine flow. Then:
Tighten (contract) the muscles you would use to stop urinating and hold for five seconds, and then relax for five seconds. (If this is too difficult, start by holding for two seconds and relaxing for three seconds.)
Work up to holding the contractions for 10 seconds at a time.
Aim for at least three sets of 10 repetitions each day.
To help you identify and contract the right muscles, your doctor may suggest that you work with a pelvic floor physical therapist or try biofeedback techniques
Medications
Medications commonly used to treat incontinence include:
Anticholinergics. These medications can calm an overactive bladder and may be helpful for urge incontinence. Examples include oxybutynin, tolterodine, darifenacin, solifenacin.
Mirabegron. Used to treat urge incontinence, this medication relaxes the bladder muscle and can increase the amount of urine your bladder can hold. It may also increase the amount you are able to urinate at one time, helping to empty your bladder more completely.
Alpha blockers. In men who have urge incontinence or overflow incontinence, these medications relax bladder neck muscles and muscle fibers in the prostate and make it easier to empty the bladder. Examples include tamsulosin, alfuzosin, silodosin.
Topical estrogen. Applying low-dose, topical estrogen in the form of a vaginal cream, ring or patch may help tone and rejuvenate tissues in the urethra and vaginal areas.
Pads and protective garments. Most products are no more bulky than normal underwear and can be easily worn under everyday clothing. Men who have problems with dribbles of urine can use a drip collector — a small pocket of absorbent padding that’s worn over the penis and held in place by close-fitting underwear.
Catheter. If you’re incontinent because your bladder doesn’t empty properly, doctor may recommend that you learn to insert a soft tube (catheter) into your urethra several times a day to drain your bladder. You’ll be instructed on how to clean these catheters for safe reuse.
Lifestyle and home remedies
Use a washcloth to clean yourself.
Allow your skin to air-dry.
Avoid frequent washing and douching because these can overwhelm your body’s natural defenses against bladder infections.
Consider using a barrier cream, such as petroleum jelly or cocoa butter, to protect your skin from urine.
Ask your doctor about special cleansers made to remove urine that may be less drying than other products.
If you have urge incontinence or nighttime incontinence, make the toilet more convenient:
Move any rugs or furniture you might trip over or collide with on the way to the toilet.
Use a night light to illuminate your path and reduce your risk of falling.
If you have functional incontinence, you might:
Keep a bedside commode in your bedroom.
Install an elevated toilet seat.
Widen an existing bathroom doorway.
Complications
Skin problems. Rashes, skin infections and sores can develop from constantly wet skin.
Urinary tract infections. Incontinence increases your risk of repeated urinary tract infections.
Impacts on your personal life. Urinary incontinence can affect your social, work and personal relationships.
Prevention
Urinary incontinence isn’t always preventable. However, to help decrease your risk:
Maintain a healthy weight
Practice pelvic floor exercises
Avoid bladder irritants, such as caffeine, alcohol and acidic foods
Eat more fiber, which can prevent constipation, a cause of urinary incontinence
Don’t smoke, or seek help to quit if you’re a smoker
It can be embarrassing to talk about bathroom habits with healthcare provider. This embarrassment shouldn’t stop you from treating incontinence, though. Often, your healthcare provider can help figure out the cause of your bladder control issue and help make it better. You don’t need to deal with it alone. Talk to your healthcare provider about the best ways to treat incontinence so that you can lead a full and active life without worrying about leakage.
Pontine hemorrhages are a common form of intracerebral hemorrhage, and usually are a result of poorly controlled long-standing hypertension, although also have other causes. When due to chronic hypertension, the stigmata of chronic hypertensive encephalopathy are often present. It carries a very poor prognosis.
The pons is the largest component of the brain stem. When blood flow to the pons becomes interrupted, it causes a pontine stroke or pons stroke. When the disruption is caused by a blood clot in particular, it’s referred to as a pontine infarction or pontine infarct.
Epidemiology
Primary pontine hemorrhage accounts for ~7.5% (range 5-10%) of hemorrhagic strokes and has an incidence of ~3 per 100,000 people.
Cause of Pontine Stroke
Pontine strokes can be classified as either ischemic or hemorrhagic.
An ischemic stroke occurs when an artery in the brain becomes blocked by a blood clot, while a hemorrhagic stroke occurs when an artery in the brain bursts. Pontine strokes make up approximately 7% of all ischemic strokes (pontine infarct) and 10% of hemorrhagic strokes.
Hypertension and diabetes are two of the most common risk factors for all ischemic strokes and especially lacunar infarcts, a type of ischemic stroke that occurs in the deep areas of the brain such as the pons.
Other common causes of pontine stroke include diseases that affect the arteries such as small artery disease, large artery atherosclerosis (when the arteries become thickened with plaque), and cardiogenic emboli (when a blood clot travels from the heart to the brain).
Clinical Presentation of Pontine Hemorrhage
Patients present with sudden and precipitous neurological deficits. Depending on the speed at which the hematoma enlarges and the exact location, presentation may include:
Decreased level of consciousness (most common)
Long tract signs including quadriparesis
Cranial nerve palsies
Seizures
Cheyne-Stokes respiration
Pin-Point Pupil
Dysarthria
Dysphagia
Locked-in syndrome: Involves paralysis of all four limbs (tetraplegia) as well as the face. The eyes are still able move. The survivor retains full cognitive function, aware of their environment but unable to interact with it except with eye movement — as long as the other areas of the pons that control eye movement were unaffected.
Pure sensory deficits
Pathology
As is the case with penetrating arteries into the basal ganglia, the penetrating arteries from the basilar artery extending into the pons are subject to lipo-hyalinosis as a result of poorly-controlled hypertension. This renders the vessel wall prone to rupture. The larger paramedian perforators are more commonly the culprit vessels.
Radiographic features of Pontine Hemorrhage
CT
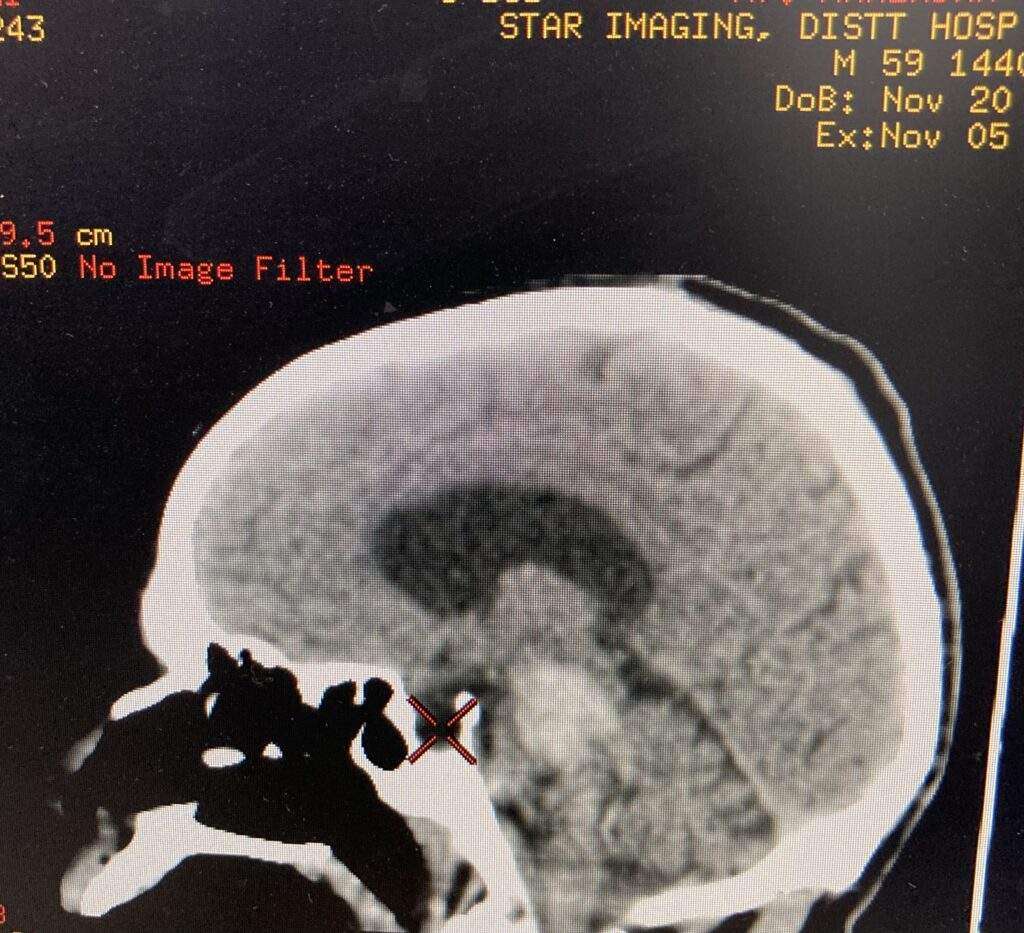
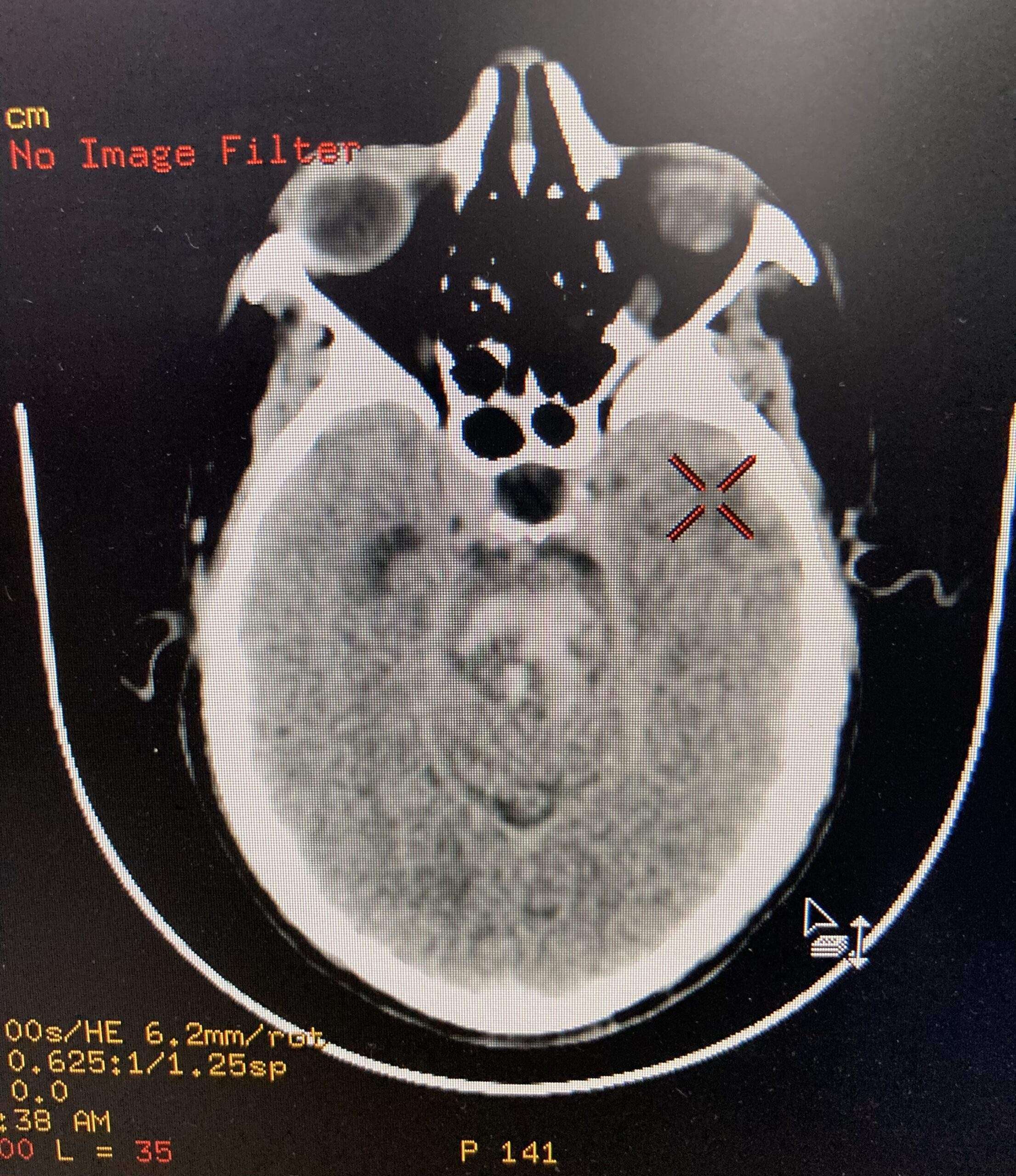
CT of the brain is usually the first, and often the only, investigation obtained upon presentation. Features typical of an acute intraparenchymal hemorrhage are noted, usually located centrally within the pons (on account of the larger paramedian perforators usually being the site of bleeding).
The hematoma more frequently extends in a rostro-caudal direction along the traversing long tracts rather than laterally into the middle cerebellar peduncle. Usually the hematoma does not extend beyond the pontomedullary junction inferiorly and the inferior midbrain superiorly. These hematomas frequently rupture into the 4th ventricle.
Pontine HemorrhagePontine Hemorrhage
MRI
In patients who have small volume bleeds and who are thought to possibly have an underlying lesion, MRI may be of use (e.g. identification of a vascular malformation).
Treatment and Prognosis
Patient with this hemorrhages have a poor prognosis, with large bleeds being almost universally fatal. Open surgical evacuation of the clot is usually not performed, although stereotactic clot aspiration has been advocated by some.
In smaller hemorrhages, medical management and treatment of hydrocephalus with extraventricular drains may be life-saving, however, often with significant residual neurological deficits.
Overall mortality ranges between 30% and 90%, with the overall volume of the bleed and initial GCS being related to outcome.
Rehabilitation for Pontine Stroke Survivors
Rehabilitation can take many forms to address the unique secondary effects caused by a pontine stroke. Therapists will help you create a custom rehabilitation plan that addresses your unique goals to improve movement and/or sensation.
One major goal of rehabilitation is to spark neuroplasticity to help rewire the brain and recover as much function as possible. Neuroplasticity is activated through massed practice as the brain gets better at the activities and skills that we repeatedly practice.
Here are some of types of therapy that are commonly used to treat the effects of a pontine stroke:
Physical Therapy
During physical therapy, your therapist will guide you through rehabilitation exercises that help improve mobility in the affected muscles. Survivors with severe motor impairments can start slow with passive range of motion exercises to help prevent complications such as contractures or pressure sores. Passive movement also helps spark neuroplasticity and rewire the brain. Over time, they may be able to progress to more active exercises and even strengthening.
Occupational Therapy
Your occupational therapist specializes in maximizing independence with the activities of daily living. Your OT will provide you with both functional exercises and any necessary compensation techniques to help you complete your daily tasks. They can also offer recommendations for home modifications to help prevent falls, discuss safety concerns and precautions following sensation loss, and provide resources for getting back to work or back to drive again.
Speech Therapy
Speech therapists are able to address difficulties with speaking, swallowing, and general communication skills. They may use a variety of exercises to improve the strength and coordination of the muscles surrounding your mouth and face. They can also suggest methods of communication other than speaking, called augmentative and alternative communication (AAC). For example, if you have locked-in syndrome, they may recommend using technology designed to track your eye movements to communicate.
Home Therapy
A strong home exercise program after stroke can make a noticeable difference during recovery. Whether you have mild, moderate, or severe effects that you wish to recover, your therapist can provide suitable exercises for you to practice at home. Home therapy is essential to keep the brain constantly stimulated and maximize neuroplasticity.
Sensory Retraining
Sometimes a pontine stroke can cause changes in sensation such as numbness, tingling, or difficulty sensing temperature. For these sensory issues, sensory retraining exercises might be able to help. It involves safely exposing your skin to various textures and temperatures to stimulate the brain.
Recovery from Pontine Stroke
Overall, a pontine stroke can affect movement and/or sensation on one or both sides of the body. Although pontine infarcts are technically small in nature, they can create significant effects such as locked-in syndrome, especially when both sides of the pons were affected.
Fortunately, with a rigorous rehabilitation regimen, survivors can stimulate the brain and maximize their chances of recovery. Not all survivors will achieve a full recovery, but it’s a possibility for many. Approach your stroke recovery prognosis with curiosity to see how far you can go.
Urinary Bladder cancer is a common type of cancer that begins in the cells of the bladder. The bladder is a hollow muscular organ in your lower abdomen that stores urine.
Urinary bladder cancer most often begins in the cells (urothelial cells) that line the inside of your bladder. Urothelial cells are also found in your kidneys and the tubes (ureters) that connect the kidneys to the bladder. Urothelial cancer can happen in the kidneys and ureters, too, but it’s much more common in the bladder.
Most bladder cancers are diagnosed at an early stage, when the cancer is highly treatable. But even early-stage bladder cancers can come back after successful treatment. For this reason, people with bladder cancer typically need follow-up tests for years after treatment to look for bladder cancer that recurs.
What are Urinary bladder Cancer types?
There are three types of urinary bladder cancer. Each type is named for the cells that line the wall of your bladder where the cancer started. Bladder cancer types include:
Transitional cell carcinoma: This cancer starts in transitional cells in the inner lining of your bladder wall. About 90% of all bladder cancers are transitional. In this cancer type, abnormal cells spread from the inner lining to other layers deep in your bladder or through your bladder wall into fatty tissues that surround your bladder. This bladder cancer type is also known as urothelial bladder cancer.
Squamous cell carcinoma: Squamous cells are thin, flat cells that line the inside of your bladder. This bladder cancer accounts for about 5% of bladder cancers and typically develops in people who’ve had long bouts of bladder inflammation or irritation.
Adenocarcinoma: Adenocarcinoma cancers are cancers in the glands that line your organs, including your bladder. This is a very rare type of bladder cancer, accounting for 1% to 2% of all bladder cancers.
Small cell carcinoma of the bladder: This extremely rare type of bladder cancer affects about 1,000 people in the U.S.
Sarcoma: Rarely, soft tissue sarcomas start in bladder muscle cells.
Healthcare providers may also categorize bladder cancer as being noninvasive, non-muscle-invasive or muscle-invasive.
Noninvasive: This bladder cancer may be tumors in a small section of tissue or cancer that’s only on or near the surface of your bladder.
Non-muscle-invasive:This refers to bladder cancer that’s moved deeper into your bladder but hasn’t spread to muscle.
Muscle-invasive:This bladder cancer has grown into bladder wall muscle and may have spread into the fatty layers or tissues on organs outside of your bladder.
Risk Factors for Urinary Bladder Cancer
Cigarette smoke: Smoking cigarettes more than doubles your risk of developing bladder cancer. Smoking pipes and cigars and being exposed to second-hand smoke may also increase your risk.
Radiation exposure: Radiation therapy to treat cancer may increase your risk of developing bladder cancer.
Chemotherapy: Certain chemotherapy drugs may increase your risk.
Exposure to certain chemicals: Studies show that people who work with certain chemicals used in dyes, rubber, leather, paint, some textiles and hairdressing supplies may have an increased risk.
Frequent bladder infections: People who have frequent bladder infections, bladder stones or other urinary tract infections may be at an increased risk of squamous cell carcinoma.
Chronic catheter use: People who have a chronic need for a catheter in their bladder may be at risk for squamous cell carcinoma.
Symptoms of Urinary Bladder Cancer
Bladder cancer signs and symptoms may include:
Blood in urine (hematuria), which is painless and may cause urine to appear bright red or cola colored, though sometimes the urine appears normal and blood is detected on a lab test
Frequent urination
Painful urination
Back pain
Diagnosis of Urinary Bladder Cancer
Urinalysis: Providers use a variety of tests to analyze your pee. In this case, they may do urinalysis to rule out infection.
Cytology: Providers examine cells under a microscope for signs of cancer.
Cystoscopy: This is the primary test to identify and diagnose bladder cancer. For this test, providers use a pencil-sized lighted tube called a cystoscope to view the inside of your bladder and urethra. They may use a fluorescent dye and a special blue light that makes it easier to see cancer in your bladder. Providers may also take tissue samples while doing cystoscopies.
If urinalysis, cytology and cystoscopy results show you have bladder cancer, healthcare providers then do tests to learn more about the cancer, including:
Transurethral Resection of Bladder Tumor (TURBT): Providers do this procedure to remove bladder tumors for additional tests. TURBT procedures may also be a treatment, removing bladder tumors before the tumors can invade your bladder’s muscle wall. This test is an outpatient procedure done under spinal or general anesthesia.
Magnetic Resonance Imaging (MRI): This imaging test uses a magnet, radio waves and a computer to take detailed images of your bladder.
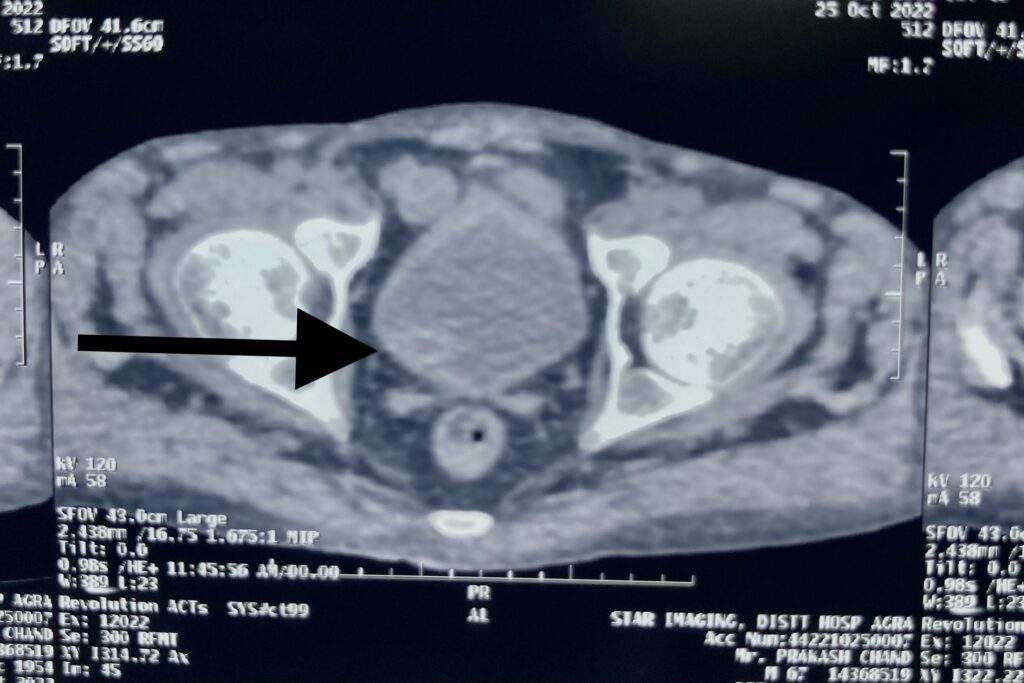
Computed Tomography (CT) Scan: Providers may do this test to see if cancer has spread outside of your bladder.
Chest X-ray: This test lets providers check for signs bladder cancer has spread to your lungs.
Bone scan: Like a chest X-ray, bone scans check for signs bladder cancer has spread to your bones.
Biopsies to look for cancer spread.
How do I take care of myself?
About half of all people with bladder cancer have early-stage cancer that’s relatively easy to treat. But bladder cancer often comes back (recurs). People who’ve had bladder cancer will need regular checkups after treatment. Being vigilant about follow-up care is one thing you can do to take care of yourself. Here are some other suggestions from the Bladder Cancer Advocacy Network include:
Follow a heart-healthy diet: Plan menus that include skinless poultry and fish, low-fat dairy products, nuts and legumes, and a variety of fruits and vegetables.
Focus on high-fiber foods: Bladder cancer treatment may cause digestive issues and a fiber-rich diet may help.
Get some exercise: Gentle exercise may help manage stress.
Connect with others: Bladder cancer often comes back. It’s not easy to have a rare disease that’s likely to return. Connecting with people who understand what you’re going through may help.
If you have bladder cancer, it may help to know about half of all people with the condition receive treatment when their tumors are limited to the inner layer of their bladder wall. For them, surgery to remove tumors means they’re cancer-free. But bladder cancer often comes back (recurs). If you’re worried about recurring cancer, talk to your healthcare provider. They’re your best resource for information on risk factors that increase the chance you’ll have another bout of bladder cancer. They’ll help you stay vigilant about symptoms that may be signs of recurring bladder cancer and be there for you if you need more bladder cancer treatment.
When someone has a stroke, every second is crucial. The longer it takes to receive treatment, the more likely it is that damage to the brain will occur.
“The mantra is ‘time is brain’. “The sooner they get treatment, the better patients do.”
World Stroke Day is recognized each year on Oct. 29. The aim is to teach the public about stroke risk factors and stroke prevention, and to raise awareness about the warning signs of stroke so people recognize when a loved one may be having a stroke and can take action.
What is Stroke?
A stroke occurs when a blood vessel bringing blood and oxygen to the brain is interrupted or ruptures (bursts) and brain cells don’t get the flow of blood that they need. Deprived of oxygen, nerve cells can’t function and die within minutes. When nerve cells do not function, the part of the body they control can’t function either. The devastating effects of stroke are often permanent because dead brain cells can’t be replaced.
Types of Stroke
There are two main types of strokes: ischemic and hemorrhagic. An ischemic stroke happens when there is a loss of blood supply to an area of the brain. A hemorrhagic stroke happens when there is bleeding into the brain when a blood vessel ruptures. Eighty-five percent of all strokes are ischemic.
Blood supply to the brain
Blood vessels that carry blood to the brain from the heart are called arteries. The brain needs a constant supply of blood, which carries the oxygen and nutrients it needs to function. Each artery supplies blood to specific areas of the brain. A stroke occurs when one of these arteries to the brain either is blocked or bursts. As a result, part of the brain does not get the blood it needs, so it starts to die.
Possible Effects of Stroke
Motor and sensory function
The human brain is divided into several areas that control movement and sensory function, or how the body moves and feels. When a stroke damages a certain part of the brain that area may no longer work as well as it did before the stroke. This can cause problems with walking, speaking, seeing or feeling.
Functions of right and left hemisphere of the brain
The left side, or hemisphere, of the brain controls how the opposite (right side) of the body moves and feels, and is responsible for how well we can figure out problems with science, understanding what we read and what we hear people say, number skills such as adding and subtracting, and reasoning. The right side of the brain controls the movements and feelings on the left side of the body and is in charge of how artistic we are, including musical and creative talents.
Stages of normal and blocked artery blood flow
Normal artery: Blood flows easily through a clear artery.
Blockage: An artery can become blocked by plaque (a fatty substance that clogs the artery) or a blood clot, which reduces blood flow to the brain and may cause a stroke.
Blockage cleared: The plaque or blood clot breaks up quickly and blood flow is restored to the brain. This may happen during a TIA or mini-stroke, where brain cells recover with no permanent brain damage.
Stroke Symptoms from “Fast to Faster” – देखना, दिखना, हाथ, पैर, बोल, चाल
Fast Stroke Symptoms – देखना, दिखना, हाथ, पैर, बोल, चाल
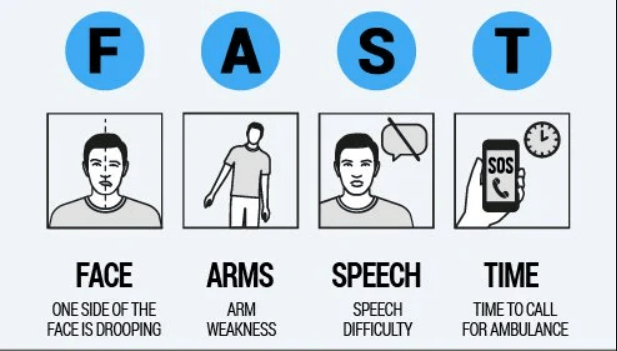
The acronym FAST (Facial drooping, Arm weakness, Speech difficulties and Time) has been used by the National Stroke Association, American Heart Association and others to educate the public on detecting symptoms of a stroke. FAST was first introduced in the United Kingdom in 1998.
Hindi version of FAST is “Dekhna, dikhna, hath, paer, bol, chal” – could be an easy mnemonic. Any sudden onset disturbance in dekhna, dikhna, hath, paer, bol or chal should raise suspicion of a cerebrovascular event and may indicate prompt medical consultation.
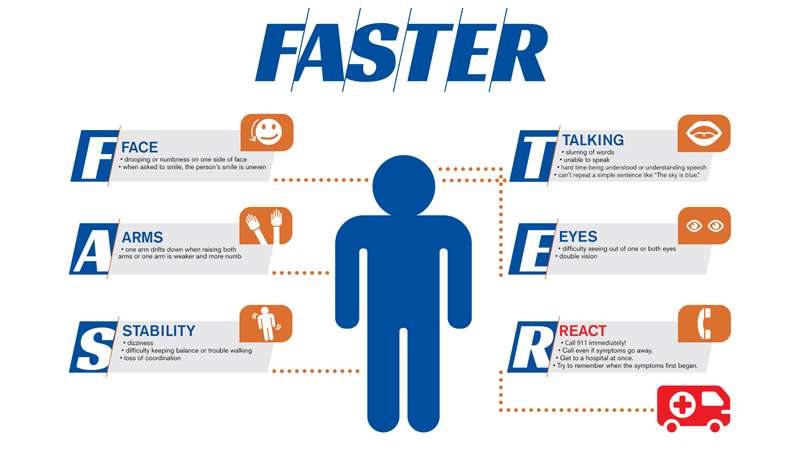
Faster Stroke Symptoms – देखना, दिखना, हाथ, पैर, बोल, चाल
F stands for Face, which refers to drooping or numbness on one side of the face versus the other. Ask the person to smile to make the droop more apparent.
A stands for Arms, which refers to one arm being weaker or more numb than the other. Ask the individual to raise both arms up and hold them for a count of ten. If one arm falls or begins to drop, then this could be a sign of a stroke.
S stands for Stability, which refers to steadiness on your feet. Sometimes individuals will fall, feel very dizzy or be unable to stand without assistance. Difficulty maintaining balance, trouble walking and loss of coordination are all possible stroke symptoms.
T stands for Talking, which refers to changes in speech including slurring, garbled, nonsensical words, or the inability to respond appropriately. Individuals experiencing a stroke may be difficult to understand, or they may have difficulty understanding others. Ask the person to repeat a simple sentence like “The sky is blue.”
E stands for Eyes, which refers to visual changes. These visual changes occur suddenly and can include complete vision loss in one eye, double vision, and partial loss of vision in one or both eyes.
R stands for React, which is a reminder to call nearby health facility immediately if you recognize any of these symptoms. Call even if the symptoms go away and try to remember when they first began..
Identifying and reacting to stroke symptoms quickly is crucial to achieving proper treatment for an individual experiencing a stroke. Recognizing these “FAST” symptoms and getting treatment quickly can minimize damage to the brain and lessen post-stroke complications.
Diagnosis of Stroke
In addition to a physical examination and laboratory tests, physicians may use a variety of advanced imaging diagnostic tests to diagnose a stroke.
In the emergency room, your doctor or stroke emergency team will:
ask you when the symptoms of the stroke started
ask you about your medical history
conduct a physical and neurological examination
order certain laboratory (blood) tests
perform imaging tests to help determine what kind of stroke you are having
request additional tests that might be needed
request additional tests that might be needed, which could include some of the following:
Imaging Tests
CT scan (computed tomography)
An imaging test of the brain that uses radiation to create a picture (like an X-ray) of the brain. It’s usually one of the first tests given to a patient with stroke symptoms as test results give valuable information about the cause of stroke and the location and extent of brain tissue affected.
MRI (magnetic resonance imaging)
An MRI uses a large magnetic field to produce an image of the brain. Like the CT scan, it shows the location and extent of brain injury. The image produced by MRI is sharp and detailed, so it’s often used to diagnose small, deep injuries and may help determine a possible cause of the stroke.
Echocardiogram
An ultrasound imaging procedure used to assess the heart’s function and structures. It can be used to check for conditions such as heart disease, congenital birth defects, heart failure, pericarditis (an inflammation of the lining of the heart) or disease of the valves which might identify the cause of the stroke.
Blood Flow Tests
Carotid artery ultrasound
A carotid artery ultrasound may be ordered if your doctor hears an abnormal sound over your carotid artery caused by disturbances in the blood flow. This diagnostic test takes images of the blood flowing through the arteries and it can detect how severe the narrowing is from plaque buildup.
Cerebral angiography/cerebral arteriography
A cerebral angiography/cerebral arteriography can be performed to diagnose and show the degree of carotid artery stenosis. This test feeds a catheter from your groin, through your aorta and into the carotid artery. An injectable contrast dye is then inserted into the artery while images of the area are captured. This dye allows your doctor to view the arteries in a more enhanced field of view to detect any vessel abnormality. This test is similar to a catheterization to the heart.
Prevention of Stroke
Many strokes can be prevented in the first place by minimizing risk factors. Maintaining a healthy body weight, staying physically active and controlling blood pressure reduce the risk of stroke. Other stroke prevention steps include stopping smoking, eating a healthy diet and managing blood sugar levels.
Clinics on cloud health kisosk is an aggregtion of CE/FDA/Medical Grade devices combined with HIPPA complaint backened software which solves problem of basic health awarness checkup.
The company has conducted 100 health machines across the state and for this, it had entered into an agreement with ‘Clinics on Round’, firm. Interestingly, this machine can be handled by anyone competently.
People will be able to get their full body check-up done in 10 minutes at a Health ATM. These health ATMs will be installed in parks, markets, hospitals and such places where there is more movement of people. Tests for dengue, malaria, HIV, typhoid will be done.
Efficiently conducting the tests to check corona infection without any help from a doctor, the Hindustan Antibiotics Company Limited (HAL) has come up with the ‘Health ATM’, a digital machine which was one of its kinds in India. The Pimpri based company HAL through this machine will conduct 22 different tests and will give the results within five minutes stating whether you are fit or unfit.
Inbuild Devices in Digital Health ATM Machine: The advanced technology
Blood pressure
Glucometer
Thermometer
Oximeter
Hemoglobinometer
Digital Height Sensor
Body fat analyser etc.
Total 22 parameters measured in digital health ATM machine:
BMI, BMR, Body fat, Body water, Bone mass fat, Free weight, Muscles mass, Protein, Skeletal muscles subcutaneous mass, Visceral fat, Weight, Physic rating, Metabolic age, Health score, Height, BP, Blood sugar level, Pulse, SPO2, Body temperature and Haemoglobin.
What all can be done
To install 100 health ATS on an experimental basis
10,000 machines to be produced in the first phase
To be given for emergency services
Immediate use in the high-risk area
To store the health information digitally
HIPPA (Health insurance portability and accountability act 1996)
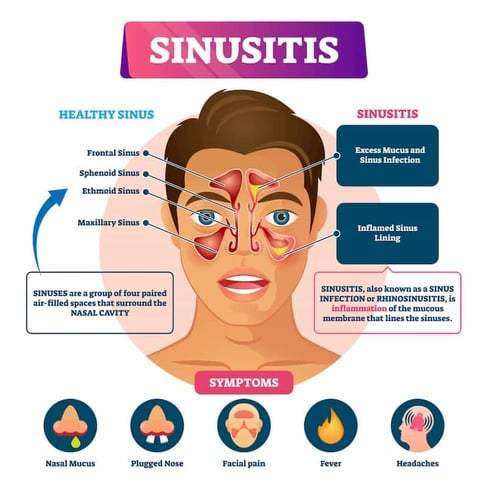
An infection of the sinuses is known as acute sinusitis. Rhinosinusitis is often a better word since the sinus passageways and nasal passages are connected. Acute rhinosinusitis is a frequent diagnosis, resulting in a significant amount of yearly healthcare costs and plenty of visits to primary care facilities. Additionally, it is a typical justification for prescribing antibiotics.
It can be brought on by bacterial, viral, or fungal infections, with viral infections being the most frequent. Antibiotics are frequently overprescribed in the treatment of this ailment, so it’s crucial to understand how to correctly examine a sinusitis patient and determine when antibiotics are necessary. In accordance with the recommendations made by several societies, this article covers the causes of rhinosinusitis and when antibiotic treatment in the management of this illness might be appropriate.
Different types of rhinosinusitis may be separated into the following categories based on consensus opinions :
Acute – Signs and symptoms for fewer than four weeks.
Subacute – It takes between four and twelve weeks for symptoms to subside.
Chronic – Enduring symptoms for more than 12 weeks.
Recurrent – Four episodes lasting fewer than four weeks, with full symptom relief between each episode.
Occurrence
One out of every five antibiotic prescriptions for adults is for acute rhinosinusitis, making it the sixth most prevalent cause for an antibiotic prescription. 6 to 7 per cent of children with respiratory symptoms are affected by acute rhinosinusitis.
Approximately,
16% of individuals are diagnosed yearly with ABRS. Given the clinical nature of this diagnosis, an overestimation is possible.
An estimated 0.5 to 2.0% of viral rhinosinusitis (VRS) in adults.
And 5 to 10% of children will progress to bacterial infections.
Causes
The most prevalent cause of acute rhinosinusitis is viruses.
The microorganisms responsible for viral rhinosinusitis (VRS) include rhinovirus, adenovirus, influenza virus, and parainfluenza virus.
Streptococcus pneumonia (38%) is the most prevalent cause of acute bacterial rhinosinusitis (ABRS), followed by Haemophilus influenzae (36%) and Moraxella catarrhalis (16%).
Rarely, fungal infections may also cause acute rhinosinusitis, although this is virtually only seen in immunocompromised people.
It is crucial to distinguish between acute invasive fungal sinusitis (IFS) and allergic fungal sinusitis (AFS), which manifests in immunocompetent people as a mass-like lesion filling a sinus canal and often causes persistent symptoms.
How to assess the patient?
1. Clinical evaluations often identify acute rhinosinusitis. The most sensitive and specific “cardinal” symptoms for acute rhinosinusitis are purulent nasal discharge accompanied by nasal obstruction or face pain/pressure/fullness. This must be determined particularly from people who report “headache” as a general complaint. Facial pressure is a symptom of sinusitis, but the headache is not (with the rare exception of sphenoid sinusitis, which may manifest as an occipital or vertex headache and is often persistent). The observant doctor must gather this information from the patient in order to ascertain the patient’s precise symptoms.
2. ABRS may be diagnosed if cardinal symptoms continue beyond ten days or if they intensify after an initial period of recovery (“double worsening”). Acute rhinosinusitis is accompanied by cough, weariness, hyposmia, anosmia, maxillary dental discomfort, and ear fullness or pressure. Mucopus coming from the osteomeatal complex may be detected by anterior rhinoscopy, or it may be proven by formal endoscopic rhinoscopy in the clinic.
3. The clinical manifestation of ABRS differs somewhat across children. Children are more likely to appear with fevers, in addition to the 10-day length, cardinal symptoms, and “double worsening.” Initial nasal discharge may be watery, then become purulent. Approximately 80% of acute bacterial sinusitis is preceded by an upper respiratory infection.
4. The severity of the symptoms suggests a bacterial origin. At the onset of the disease, these symptoms include high fevers (above 39 C or 102 F) accompanied by purulent nasal discharge or face discomfort for three to four consecutive days. Generally, viral diseases resolve within three to five days.
Antibiotic resistance issues must also be taken into account. These include:
Antibiotic usage during the past month
Hospitalisation within the preceding five days
Healthcare profession
Local antibiotic resistance trends are known to local healthcare providers
Finally, it is important to determine whether a patient is at increased risk. Included among these attributes are:
Comorbidities (i.e., cardiac, renal, or hepatic disease)
Immunocompromised states
Age under 2 years or over 65 years
5. In immunocompromised patients, acute fungal rhinosinusitis is often accompanied by fevers, nasal blockage or bleeding, and face discomfort; however, it may also be asymptomatic. Refractory or severe symptoms should urge investigation of this diagnosis in immunocompromised patients.
How to diagnose the condition?
Clinical evaluations often identify acute rhinosinusitis. It is essential for the doctor to differentiate between VRS and ABRS in order to guarantee the appropriate use of antibiotics.
Local resistance patterns and prevalence of penicillin non-susceptible S. pneumoniae warrants clarification.
The conventional diagnostic criteria for adult rhinosinusitis include the presence of at least two significant symptoms or one major symptom plus two or more mild symptoms. In youngsters, the requirements are the same, with the exception of a greater focus on nasal discharge (rather than nasal obstruction).
Principal Symptoms :
Purulent anterior nasal discharge
Fever (for acute sinusitis only)
Purulent or discoloured posterior nasal discharge
Facial congestion or fullness
Nasal congestion or obstruction
Facial pain or pressure
Hyposmia or anosmia
Mild features:
Headache
Ear pain or pressure or fullness
Halitosis
Dental pain
Cough
Fever (for subacute or chronic sinusitis)
Fatigue
Here is some clinical advice for telling ABRS from VRS:
Duration of symptoms exceeding 10 days.
At the onset of the disease, a high temperature (above 39 C or 102 F) is accompanied by purulent nasal discharge or face discomfort for three to four consecutive days.
Increase in symptom severity within the first 10 days.
In general, routine laboratory testing is unnecessary. Evaluations for cystic fibrosis, ciliary dysfunction, and immunodeficiency should be considered for chronic, recurring, or persistent rhinosinusitis. Some data suggest that a high ESR and CRP may indicate a bacterial infection.
The gold standard is the culture of endoscopic aspirates with more than or equal to 10 CFU/mL. However, this is not required for ABRS diagnosis and is not performed in the great majority of instances. Due to their weak connection with endoscopic aspirates, nasal and nasopharyngeal cultures are of little value. Referral for endoscopic aspiration may be beneficial for individuals with resistant infections or numerous antibiotic sensitivities.
Imaging is rarely indicated for acute sinusitis unless there is clinical concern for a complication or alternate diagnosis. Plain sinus films are often ineffective in identifying inflammation. They may display air-fluid levels. However, this does not aid in distinguishing between viral and bacterial etiologies. If a complication or other diagnosis is suspected, or if the patient has repeated acute infections, sinus CT imaging should be performed to evaluate for bone, soft tissue, dental, or other structural abnormalities, as well as chronic sinusitis.
These should be attained after an acceptable course of therapy. CT scans of the sinuses may reveal air-fluid levels, opacification, and inflammation. Over 5 mm of thicker sinus mucosa is symptomatic of inflammation. Additionally, it can efficiently evaluate bone deterioration or disintegration. However, these data are not useful for distinguishing between viral and bacterial etiologies.
MRI provides more information than sinus CT when evaluating soft tissue or illuminating a malignancy. Consequently, MRI may be useful for determining the severity of problems in situations involving ocular or cerebral extension.
How to manage the condition?
Antibiotic medication or a period of cautious waiting may be used to treat ABRS, provided that reliable follow-up is assured. There are minor differences in the guidelines of various expert committees.
The amended 2015 American Academy of Otolaryngology Adult Sinusitis guideline suggests amoxicillin with or without clavulanate for 5 to 10 days as first-line treatment for the majority of people. Failure of treatment is determined if symptoms do not improve or worsen within seven days.
The Infectious Disease Society of America Guidelines for Acute Bacterial Rhinosinusitis prescribe amoxicillin with clavulanate for 10 to 14 days in children and 5 to 7 days in adults as first-line treatment. Failure of treatment is determined if symptoms do not improve within 3 to 5 days or worsen within 48 to 72 hours.
theAmerican Academy of Pediatrics Clinic Practice Guideline for the diagnosis and management of acute bacterial sinusitis in children aged 18 years recommended amoxicillin with or without clavulanate as first-line treatment. Uncertainty surrounds the length of therapy, although their recommendation was to continue treatment for a further seven days after symptoms disappear.
If, after 72 hours of therapy, symptoms do not improve or worsen, the treatment has failed. If the patient cannot accept oral fluids, ceftriaxone 50 mg/kg may be administered. If the patient can tolerate oral fluids the next day and improves, he or she may then begin an oral antibiotic regimen. To effectively address beta-lactamase-producing bacteria, a separate article recommends amoxicillin with clavulanate as the first treatment for children.
Adding clavulanate or prescribing high-dose amoxicillin (90mg/kg/day vs 45mg/kg/day) in children is determined by local antibiotic resistance trends, the patient’s risk level, risk factors for antibiotic resistance, and the severity of symptoms.
A third-generation cephalosporin with clindamycin (for enough coverage of non-susceptible S. pneumoniae) or doxycycline might be therapeutic options for penicillin-allergic individuals. The effectiveness of third-generation cephalosporins alone against S. pneumoniae is inconsistent. Fluoroquinolones might also be explored, although they have a greater incidence of adverse effects. In youngsters, doxycycline and fluoroquinolones should be administered with more care. S. pneumoniae and Hemophilus influenzae have elevated levels of resistance to second-generation cephalosporins, trimethoprim/sulfamethoxazole, and macrolides.
There is also evidence that antibiotic medication does not always reduce the duration of symptoms or the risk of complications in adults. Many instances of ABRS may also resolve spontaneously within two weeks.
Symptomatic therapies
Clinicians may give symptomatic therapies, but generally, there is a lack of conclusive data. In guidelines, nasal steroids and nasal saline irrigation are the most popular suggestions. By lowering mucosal oedema, intranasal steroids may assist in relieving the blockage. A limited number of clinical studies suggested that greater dosages of intranasal corticosteroids may reduce the period of symptom remission by two to three weeks. Additionally, nasal saline irrigation may aid in reducing blockage. Due to their ability to thicken nasal secretions, antihistamines are not recommended unless there is a definite allergic component.
Be aware of potential complications
Complications are uncommon, occurring in around one out of every thousand cases. Infections of the sinuses may extend to the orbit, bone, and cerebral cavities. 80% of orbitocranial problems manifest in the orbit. These problems may be associated with substantial morbidity and death. Due to the very thin ethmoid bone that divides infections from the ethmoid from the orbit, the orbit is the most likely location.
Prognosis
Most cases of acute bacterial rhinosinusitis are viral. The vast majority of cases are either self-limiting or efficiently treatable with antibiotics. In immunocompromised individuals, invasive fungal rhinosinusitis is an uncommon but severe type of illness. It is related to a high risk of morbidity and death.
It is a viral infection that causes an outbreak of a painful rash or blisters on the skin. It’s caused by the varicella-zoster virus, which is the same virus that causes chickenpox. The rash most often appears as a band of rashes or blisters in one area of your body.
Where does it come from?
When you have chickenpox as a child, your body fights off the varicella-zoster virus and the physical signs of chickenpox fade away, but the virus always remains in your body. In adulthood, sometimes the virus becomes active again. This time, the varicella-zoster virus makes its second appearance in the form of shingles.
How common is shingles?
About 1 million cases are diagnosed every year. The risk of shingles increases as you get older, with about half the cases occurring in people over the age of 50. Shingles develops in about 10% of people who have had chickenpox at an earlier time in their lives.
Who is at risk for getting shingles?
People who have had chickenpox who are more likely to develop shingles include those:
With a weakened immune system (such as people with cancer, HIV, organ transplant recipients or those receiving chemotherapy).
Over the age of 50.
Who have been ill.
Who have experienced trauma.
Who are under stress.
The chickenpox virus doesn’t leave your body after you have chickenpox. Instead, the virus stays in a portion of your spinal nerve root called the dorsal root ganglion. For the majority of people, the virus stays there quietly and doesn’t cause problems. Researchers aren’t always sure why the virus gets reactivated, but this typically occurs at times of stress.
Can you get shingles more than once?
Yes, you can get shingles more than one time. One of the biggest myths about shingles is that it can only happen once. This isn’t true. You can have more than one episode. If you get shingles again, you usually don’t get the rash in the same place.
What are the symptoms?
Early symptoms may include:
Fever.
Chills.
Headache.
Feeling tired.
Sensitivity to light.
Stomach upset.
Other signs and symptoms that appear a few days after the early symptoms include:
An itching, tingling or burning feeling in an area of your skin.
Redness on your skin in the affected area.
Raised rash in a small area of your skin.
Fluid-filled blisters that break open then scab over.
Mild to severe pain in the area of skin affected.
How long does a shingles outbreak last?
It can take three to five weeks from the time you begin to feel symptoms until the rash totally disappears.
First, a few days before the rash appears, you may feel pain in an area on your skin. The pain is described as itching, burning, stabbing or shooting. This usually happens before the rash comes.
Next, the raised rash appears as a band or a patch, usually on one side of your body. The rash usually appears around your waistline or on one side of your face, neck, or on the trunk (chest/abdomen/back), but not always. It can occur in other areas including your arms and legs.
Within three to four days, the rash develops into red, fluid-filled, painful, open blisters.
Usually, these blisters begin to dry out and crust over within about 10 days.
The scabs clear up about two to three weeks later.
Do you always get the typical rash if you have shingles?
Occasionally, some people don’t get a rash. If you have any of the other symptoms (even without a rash), see your healthcare provider sooner rather than later. There are effective treatments you can take early for shingles. Even if you don’t have shingles, seeing your healthcare provider will help you get your condition diagnosed and treated.
Why does shingles appear mostly on one side or in one area of your body?
The virus travels in specific nerves, so you will often see shingles occur in a band on one side of your body. This band corresponds to the area where the nerve transmits signals. These rash stays somewhat localized to an area. It doesn’t spread over your whole body. Your torso is a common area, as is your face.
Is shingles contagious?
Someone can’t spread shingles to another person, but they can spread chickenpox. The varicella-zoster virus is spread through direct skin-to-skin contact with the fluid that oozes from the blisters. Shingles is rarely spread by breathing in the varicella-zoster virus the way airborne viruses are spread. If your rash is in the blister phase, stay away from those who haven’t had chickenpox or the chickenpox vaccine and keep your rash covered.
How long are you contagious if you have shingles?
If you have such lesion, you’re contagious until the rash is dried and crusted over. The varicella-zoster virus can only cause chickenpox in someone who has never had chickenpox or hasn’t been vaccinated against chickenpox.
How is shingles diagnosed?
It can be diagnosed by the way the rash is distributed on your body. The blisters of a shingles rash usually appear in a band on one side of your body. It may also be diagnosed in a laboratory using scrapings or a swab of the fluid from the blisters.
How is shingles treated?
There is no cure for shingles but there are treatments for managing the symptoms.
Antiviral medications
These drugs may ease the discomfort and make the symptoms stop sooner, particularly if you start them within 72 hours of the first sign of shingles. They may also help prevent the pain that can happen months and years later, called post-herpetic neuralgia. These medications include:
Acyclovir.
Famciclovir.
Valacyclovir.
Over-the-counter pain medications
These medications include the following and may be effective in relieving pain:
Acetaminophen.
Ibuprofen.
Other medications
Antibacterial drugs may be prescribed if you develop a bacterial infection due to the shingles rash. Anti-inflammatory drugs like prednisone may be prescribed if shingles affects your eyes or other parts of your face.
If you have more than one area of blisters, what can you expect if you go to the hospital?
It’s important to note that most people with shingles don’t need to be in a hospital, but if you do:
You’ll be in a contact isolation room.
The door will be kept closed.
A sign on your door will remind people who have never had chickenpox or the vaccine not to enter.
The sign will also remind staff to wear gowns and gloves when entering the room.
If you have shingles in only one area of your body that can’t be kept covered, what can you expect for your hospital stay?
You will be in a contact isolation room.
The sign on the door will remind staff to wear gowns and gloves when entering the room.
What are the complications of shingles?
After the shingles rash has disappeared, you might continue to have nerve pain in that same area. Post-herpetic neuralgia can last for months or years and become quite severe.
More than 10% of people who get shingles develop post-herpetic neuralgia. Researchers don’t know why some people get post-herpetic neuralgia and others don’t. It may be that nerves become more sensitive or that the virus may be invading and damaging the central nervous system.
Other complications include:
Other types of nerve issues like numbness or itching.
A bacterial infection of the shingles rash.
Eye and ear inflammation if the rash is near these organs.
Is shingles dangerous or even fatal?
If shingles involves your eye, it can lead to blindness. In rare cases, shingles can lead to hearing problems, pneumonia, inflammation of the brain (encephalitis) and even death.
How is post-herpetic neuralgia treated?
Treatments include lotions or creams (such as lidocaine or capsaicin) and/or other medications not specifically used for pain, such as antidepressants or drugs for epilepsy. Regular pain relievers are not usually effective for this type of pain.
If your pain doesn’t lessen, you might try therapies like nerve blocks or steroid injections near the area where the nerves exit the spine. Your provider might suggest an implantable nerve stimulator device for severe, ongoing pain that hasn’t responded to other treatments.
Is a vaccine available to prevent shingles?
Two vaccines are available in the market to reduce your chance of developing shingles and post-herpetic neuralgia. One vaccine, Zostavax®, has been available since 2006. The second vaccine, Shingrix®, has been available since 2017. Shingrix is recommended as the preferred vaccine by the Advisory Committee on Immunization Practices, a group of medical and public health experts.
Shingrix (recombinant zoster vaccine) is given as a two-dose shot in your upper arm. You should receive the second dose (shot) two to six months after receiving the first. Shingrix has been shown to be more than 90% effective in preventing shingles and postherpetic neuralgia. Its effectiveness remains above 85% for at least four years after receiving the vaccine.
Who should be vaccinated with Shingrix?
The Shingrix vaccine is recommended for those 50 years of age and older who are in good health.
You should get the Shingrix vaccine even if:
You’ve had shingles already.
You’ve been previously vaccinated with Zostavax (a live zoster vaccine). If you’ve been vaccinated with Zostavax, wait at least eight weeks before getting vaccinated with Shingrix.
You don’t know for sure if you’ve ever had chickenpox.
Ask your healthcare provider, who knows your entire health history if getting this vaccine is right for you.
Who should not be vaccinated with Shingrix?
You shouldn’t receive the Shingrix vaccine if you:
Have ever had a severe allergy to this vaccine or any ingredient in this vaccine.
Are breastfeeding or pregnant.
Currently have shingles.
Are ill and have a high fever.
Have tested negative for immunity to varicella-zoster virus (get the chickenpox vaccine instead).
Ask your healthcare provider if the benefits of getting the vaccine outweigh any potential risks.
What serious side effects should you watch for after getting the Shingrix vaccine?
Serious side effects from vaccines are extremely rare. However, call or go to the nearest emergency room right away if you experience any of the following within minutes to hours after receiving Shingrix:
Swelling of your face or throat.
Difficulty breathing.
Hives.
Fast heartbeat.
Dizziness, lightheadedness, weakness.
If you’ve had shingles recently, how long should you wait before getting the Shingrix vaccine?
You can get the Shingrix vaccine any time after the shingles rash has gone away.
When is it safe to return to work if you have shingles?
You can return to work when you feel well enough to return and you’re no longer contagious. This means that your blistered rash has dried up and scabbed over. This usually takes up to 10 days from the time the rash first appears.
Are there natural ways to boost your immune system to help lessen the chances of developing shingles?
Stress is a risk factor for developing it, so limiting your stress can be helpful. Try meditation, yoga or other relaxation methods.
Other things you can do include:
Eat a healthy diet.
Maintain a healthy weight.
Exercise regularly.
Aim for seven to nine hours of sleep each night.
Don’t smoke or use tobacco products.
These are all tips for an overall healthy lifestyle, not just for reducing your chance of getting shingles.
What is the difference between herpes zoster and varicella-zoster?
Herpes zoster is simply another medical name for shingles. Varicella-zoster is the virus that causes both shingles and chickenpox.
If you’ve had chickenpox, you’re at risk of developing shingles later in life. It causes a rash that is contagious and painful. The disease can have serious complications. The best thing you can do to reduce your risk is to get the shingles vaccine. The vaccines are safe and effective.
A urinary catheter is a medical device made from a thin, hollow tube that can be inserted through the urethra or through a small opening in the abdomen, in order to drain urine from the bladder. Male external catheters, though they share a similar name, are shaped like a condom and are designed to slip over the penis rather than being inserted into the body.
How does a urinary catheter work?
The hollow tube has openings at the end, so that when it is inserted into the bladder, the urine will naturally flow out through the tube into a collection bag or the toilet. Male external catheters have an adhesive that creates a leak-proof seal around the penis with an opening at the end so the urine will flow out the front, through a tube and into a collection bag.
How is the urinary catheter inserted?
Indwelling catheters will be inserted by a medical professional through the urethra or though a small opening in the abdomen in the case of suprapubic catheters. Intermittent catheters are inserted into the urethra and this can be done by yourself at home, or by a nurse or caregiver.
How do urinary catheters stay in?
Once an indwelling catheter is inserted into the bladder, an area near the end of the catheter can be inflated with sterile water, like a balloon. This small balloon is much bigger than the urethra so it holds the catheter in place, preventing it from slipping out and still allowing urine to drain through the tube in the middle of the balloon. The balloon can be deflated when the catheter is removed. Keep in mind, not all catheters stay in. Intermittent catheters are inserted only when the bladder is full, quickly draining the bladder and then removed when the bladder has emptied.
Why are urinary catheters used?
There are a great variety of diagnoses that would result in the need of a catheter. Sometimes a catheter is needed only temporarily during hospitalization. Often times they are used permanently when the bladder does not function normally or when the bladder cannot be controlled. Catheters may be used as a solution for bladder retention (inability to empty the bladder) or bladder incontinence (inability to control the bladder).
There are three main types of catheters: indwelling catheters, intermittent catheters, and external catheters for men. Catheters come in different materials, with differently shaped tips based on the user’s needs. More information on the types of catheters can be found below.
Indwelling urinary catheters
Indwelling catheters are designed to be inserted through the urethra (Foley catheter) or a small opening in the abdomen (suprapubic catheter). Indwelling catheters are designed to stay inside the body to continuously drain the bladder. Indwelling catheters are inserted by a medical professional and can be used long term, with the catheter being changed monthly.
Intermittent urinary catheters
Intermittent catheters are also known as “in and out” catheters because they are inserted and removed around 5 times a day. When inserted, they are designed to drain the bladder all at once and then be removed. The insertion of an intermittent catheter can be done in the home once the user learns the technique and has had a little practice. There are different variations of intermittent catheters, explained below.
Straight intermittent catheter: This catheter can be made from latex or silicone, is generally used with lubricant, and has a funnel at the end to drain into the toilet. This is the standard intermittent catheter.
Closed system catheters: These come pre-lubricated and are attached to a collection bag. The system is sterile and touch-free, which can help prevent infections. The urine drains into the collection bag and then is disposed of, allowing for convenient catheterization when there is not a restroom nearby.
Hydrophilic coated catheters: Catheters coated with a slippery surface that is activated with water. This eliminates the need for a separate lubricant and may reduce irritation to the urethra for frequent catheter users.
Male External Catheters, a.k.a. Condom Catheters
Male external catheters are also known as condom catheters, Texas catheters, or “gizmos.” These are different from the other catheters because they are external, so they are not inserted into the body. These catheters fit like a condom, so they can be slipped over the penis in the same way. Usually they will have an adhesive that seals against the skin of the penis, preventing leakage.
A tube connects to the front of the catheter, allowing the urine to flow out into a collection bag. Male external catheters are generally used for continuous draining of the bladder. They can be used at home with proper training, or a medical professional can change it for you. Male external catheters should be changed daily.