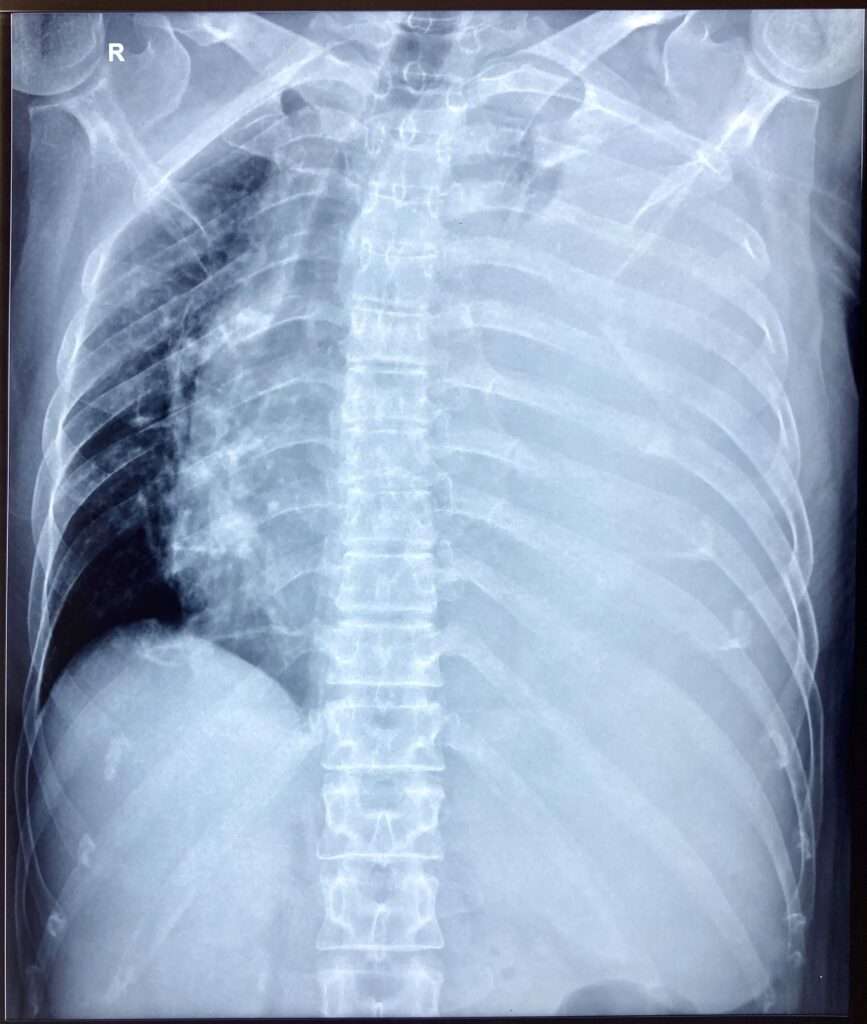
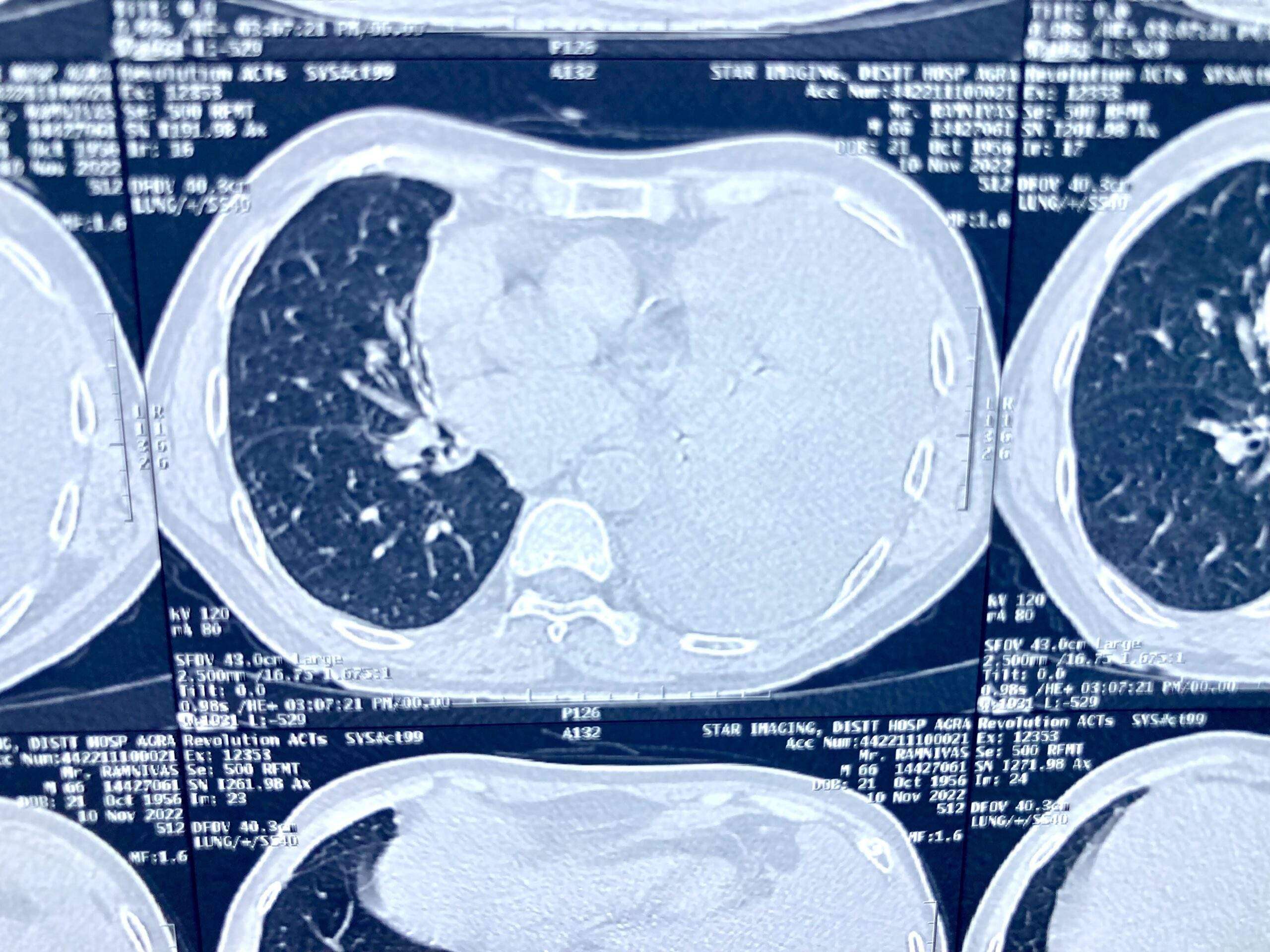
Pleural effusion, sometimes referred to as “water on the lungs,” is the build-up of excess fluid between the layers of the pleura outside the lungs. The pleura are thin membranes that line the lungs and the inside of the chest cavity and act to lubricate and facilitate breathing. Normally, a small amount of fluid is present in the pleura.
Pleural effusionPleural Effusion Aspiration Site
Symptoms
Some patients with pleural effusion have no symptoms, with the condition discovered on a chest X-ray that is performed for another reason. The patient may have unrelated symptoms due to the disease or condition that has caused the effusion. Symptoms of pleural effusion include:
Chest pain
Dry, non-productive cough
Dyspnea (shortness of breath, or difficult, labored breathing)
Orthopnea (the inability to breathe easily unless the person is sitting up straight or standing erect)
Causes
The most common causes of transudative (watery fluid) pleural effusions include:
Heart Failure
Pulmonary Embolism
Cirrhosis
Post open heart surgery
Exudative (protein-rich fluid) pleural effusions are most commonly caused by:
Pneumonia including Tuberculosis
Cancer
Pulmonary Embolism
Kidney Disease
Inflammatory disease
Other less common causes of pleural effusion include:
Autoimmune disease
Bleeding (due to chest trauma)
Chylothorax (due to trauma)
Rare chest and abdominal infections
Asbestosis pleural effusion (due to exposure to asbestos)
Meig’s syndrome (due to a benign ovarian tumor)
Ovarian hyperstimulation syndrome
Certain medications, abdominal surgery and radiation therapy may also cause it. It may occur with several types of cancer including lung cancer, breast cancer and lymphoma. In some cases, the fluid itself may be malignant (cancerous), or may be a direct result of chemotherapy.
Diagnosis
The tests most commonly used to diagnose and evaluate include:
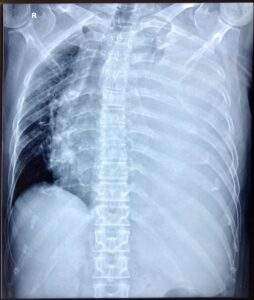
Chest X-ray
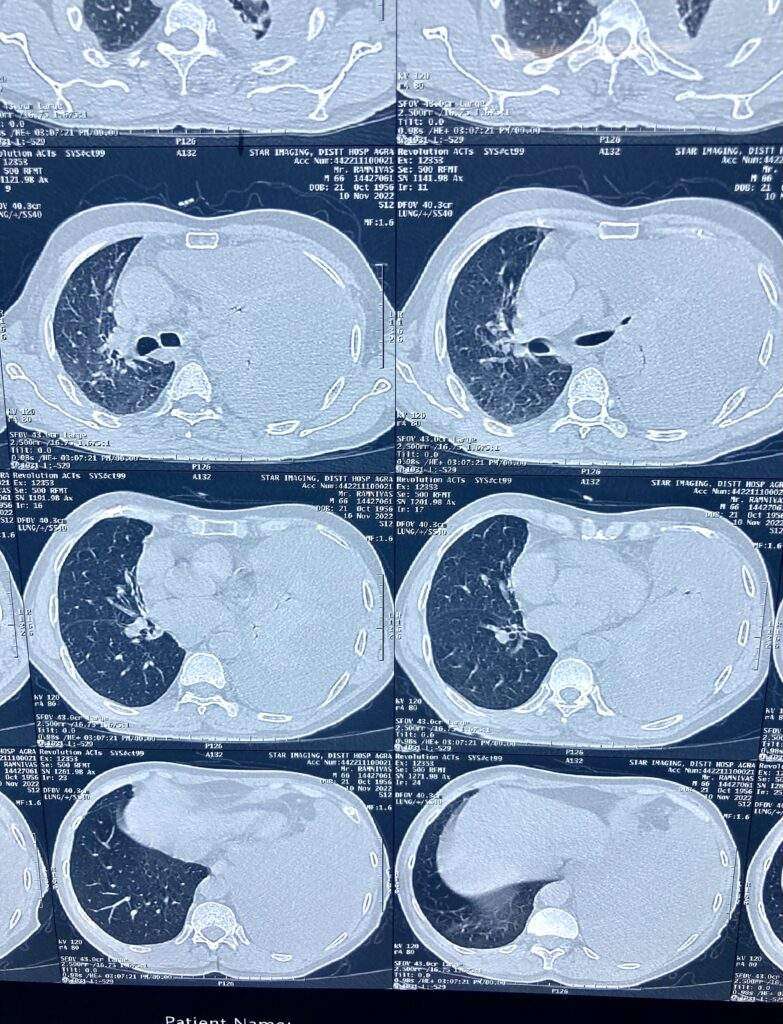
Computed Tomography (CT) of the chest
Ultrasonography of the chest
Thoracentesis (a needle is inserted between the ribs to remove a biopsy, or sample of fluid)
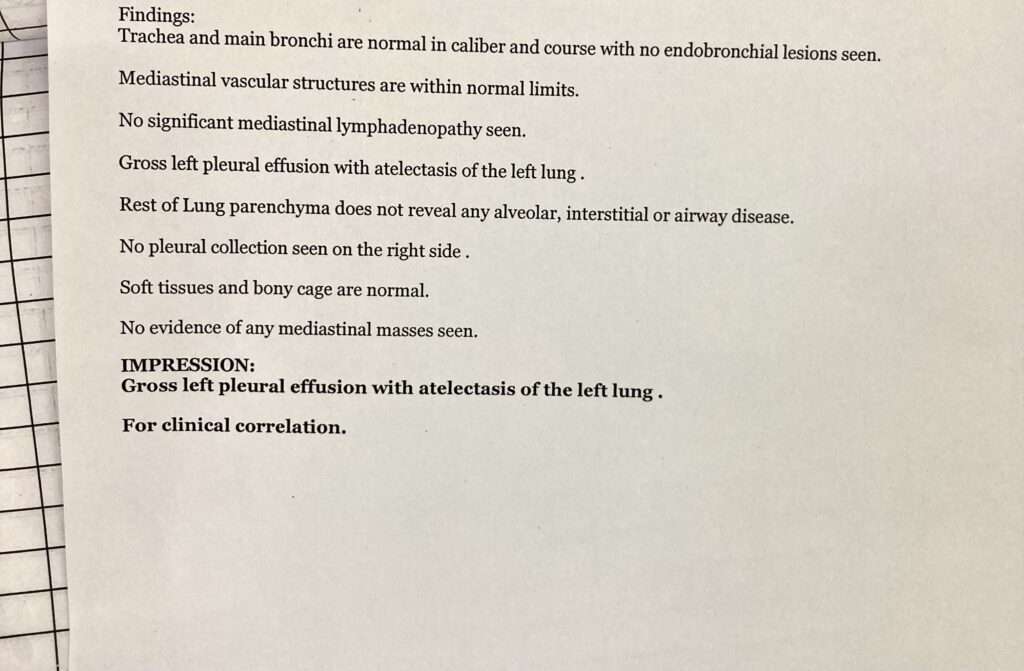
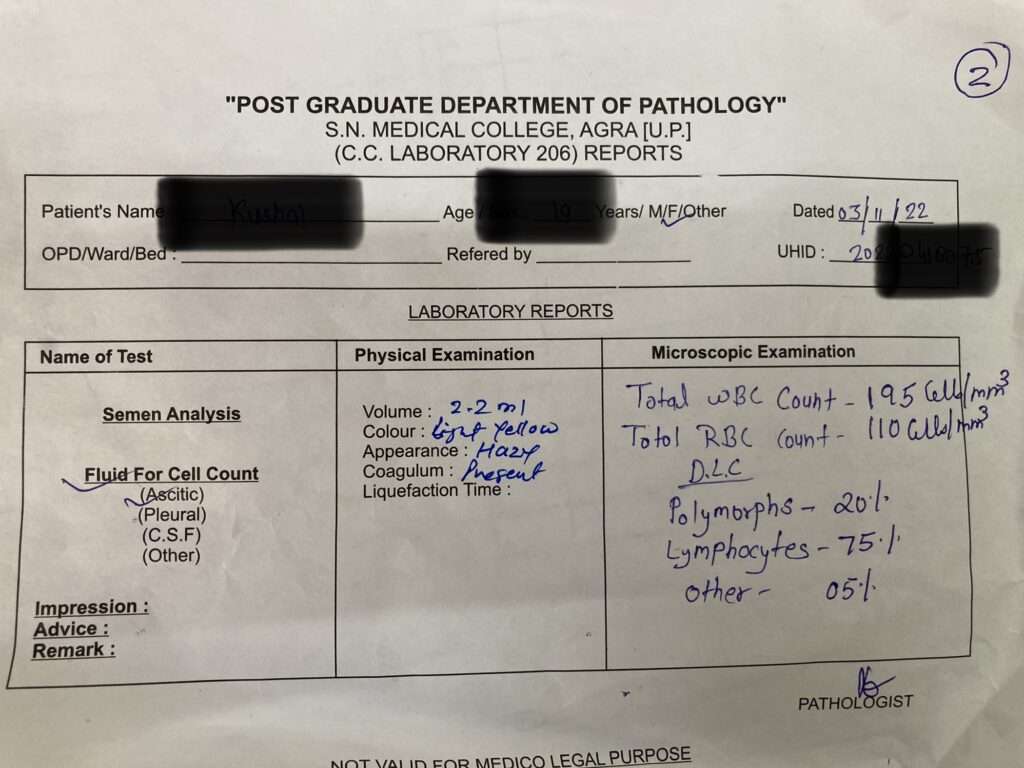
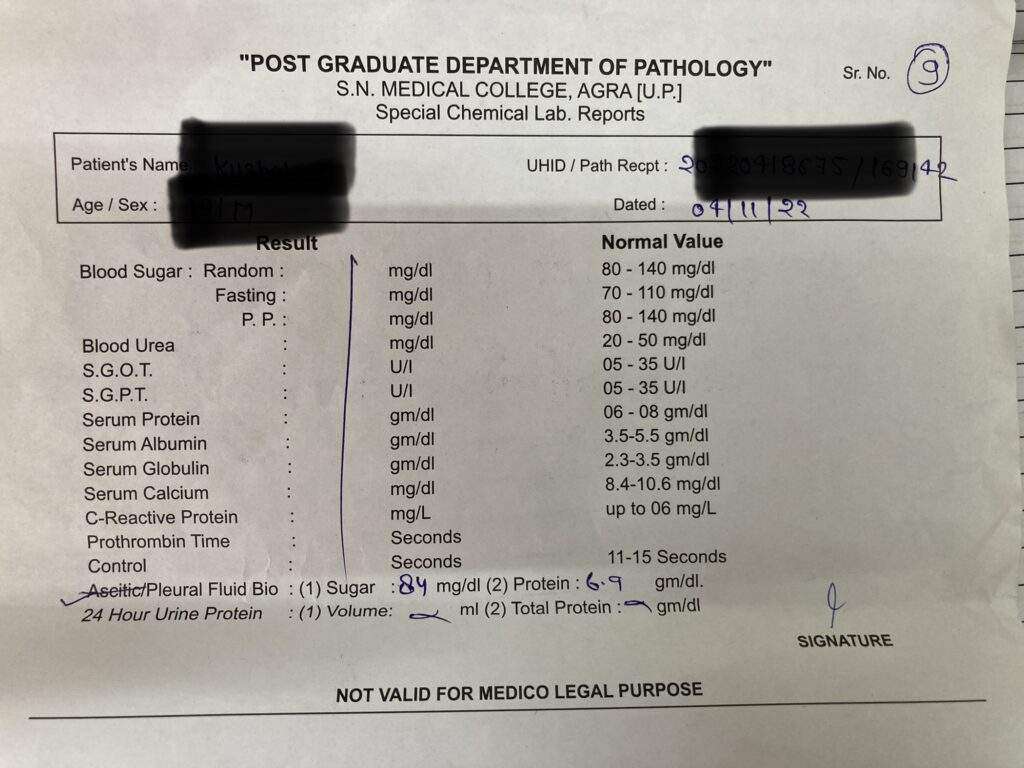
Pleural fluid analysis (an examination of the fluid removed from the pleura space)
Left Sided Massive Pleural Effusion with Mediastinal ShiftingPleural Effusion Fluid Aspiration (Diagnostic)
When it has remained undiagnosed despite previous, less-invasive tests, thoracoscopy may be performed. Thoracoscopy is a minimally invasive technique, also known as video-assisted thoracoscopic surgery, or VATS, performed under general anesthesia that allows for a visual evaluation of the pleura). Often, treatment of the effusion is combined with diagnosis in these cases.
Treatment
Treatment is based on the underlying condition and whether the effusion is causing severe respiratory symptoms, such as shortness of breath or difficulty breathing.
Diuretics and other heart failure medications are used to treat pleural effusion caused by congestive heart failure or other medical causes. A malignant effusion may also require treatment with chemotherapy, radiation therapy or a medication infusion within the chest.
A pleural effusion that is causing respiratory symptoms may be drained using therapeutic thoracentesis or through a chest tube (called tube thoracostomy).
For patients who that are uncontrollable or recur due to a malignancy despite drainage, a sclerosing agent (a type of drug that deliberately induces scarring) occasionally may be instilled into the pleural cavity through a tube thoracostomy to create a fibrosis (excessive fibrous tissue) of the pleura (pleural sclerosis).
Pleural sclerosis performed with sclerosing agents (such as talc, doxycycline, and tetracycline) is 50 percent successful in preventing the recurrence of pleural effusions.
Surgery
If cannot be managed through drainage or pleural sclerosis may require surgical treatment.
The two types of surgery include:
Video-assisted thoracoscopic surgery (VATS)
A minimally-invasive approach that is completed through 1 to 3 small (approximately ½ -inch) incisions in the chest. Also known as thoracoscopic surgery, this procedure is effective in managing pleural effusions that are difficult to drain or recur due to malignancy. Sterile talc or an antibiotic may be inserted at the time of surgery to prevent the recurrence of fluid build-up.
Thoracotomy (Also referred to as traditional, “open” thoracic surgery)
A thoracotomy is performed through a 6- to 8-inch incision in the chest and is recommended for pleural effusions when infection is present. A thoracotomy is performed to remove all of the fibrous tissue and aids in evacuating the infection from the pleural space. Patients will require chest tubes for 2 days to 2 weeks after surgery to continue draining fluid.
Surgeon will carefully evaluate you to determine the safest treatment option and will discuss the possible risks and benefits of each treatment option.
Ascites is a condition in which fluid collects in spaces within your abdomen. If severe, ascites may be painful. The problem may keep you from moving around comfortably. Ascites can set the stage for an infection in your abdomen. Fluid may also move into your chest and surround your lungs. This makes it hard to breathe.
Indications for Ascitic Fluid Tap (Abdominal Paracentesis)
To aid diagnosis of the cause of ascites or in the diagnosis or exclusion of SBP
A diagnostic paracentesis should be performed in all patients with new onset grade 2 or 3 ascites, and in all patients hospitalized for worsening of ascites or any complication of cirrhosis
Pontine hemorrhages are a common form of intracerebral hemorrhage, and usually are a result of poorly controlled long-standing hypertension, although also have other causes. When due to chronic hypertension, the stigmata of chronic hypertensive encephalopathy are often present. It carries a very poor prognosis.
The pons is the largest component of the brain stem. When blood flow to the pons becomes interrupted, it causes a pontine stroke or pons stroke. When the disruption is caused by a blood clot in particular, it’s referred to as a pontine infarction or pontine infarct.
Epidemiology
Primary pontine hemorrhage accounts for ~7.5% (range 5-10%) of hemorrhagic strokes and has an incidence of ~3 per 100,000 people.
Cause of Pontine Stroke
Pontine strokes can be classified as either ischemic or hemorrhagic.
An ischemic stroke occurs when an artery in the brain becomes blocked by a blood clot, while a hemorrhagic stroke occurs when an artery in the brain bursts. Pontine strokes make up approximately 7% of all ischemic strokes (pontine infarct) and 10% of hemorrhagic strokes.
Hypertension and diabetes are two of the most common risk factors for all ischemic strokes and especially lacunar infarcts, a type of ischemic stroke that occurs in the deep areas of the brain such as the pons.
Other common causes of pontine stroke include diseases that affect the arteries such as small artery disease, large artery atherosclerosis (when the arteries become thickened with plaque), and cardiogenic emboli (when a blood clot travels from the heart to the brain).
Clinical Presentation of Pontine Hemorrhage
Patients present with sudden and precipitous neurological deficits. Depending on the speed at which the hematoma enlarges and the exact location, presentation may include:
Decreased level of consciousness (most common)
Long tract signs including quadriparesis
Cranial nerve palsies
Seizures
Cheyne-Stokes respiration
Pin-Point Pupil
Dysarthria
Dysphagia
Locked-in syndrome: Involves paralysis of all four limbs (tetraplegia) as well as the face. The eyes are still able move. The survivor retains full cognitive function, aware of their environment but unable to interact with it except with eye movement — as long as the other areas of the pons that control eye movement were unaffected.
Pure sensory deficits
Pathology
As is the case with penetrating arteries into the basal ganglia, the penetrating arteries from the basilar artery extending into the pons are subject to lipo-hyalinosis as a result of poorly-controlled hypertension. This renders the vessel wall prone to rupture. The larger paramedian perforators are more commonly the culprit vessels.
Radiographic features of Pontine Hemorrhage
CT
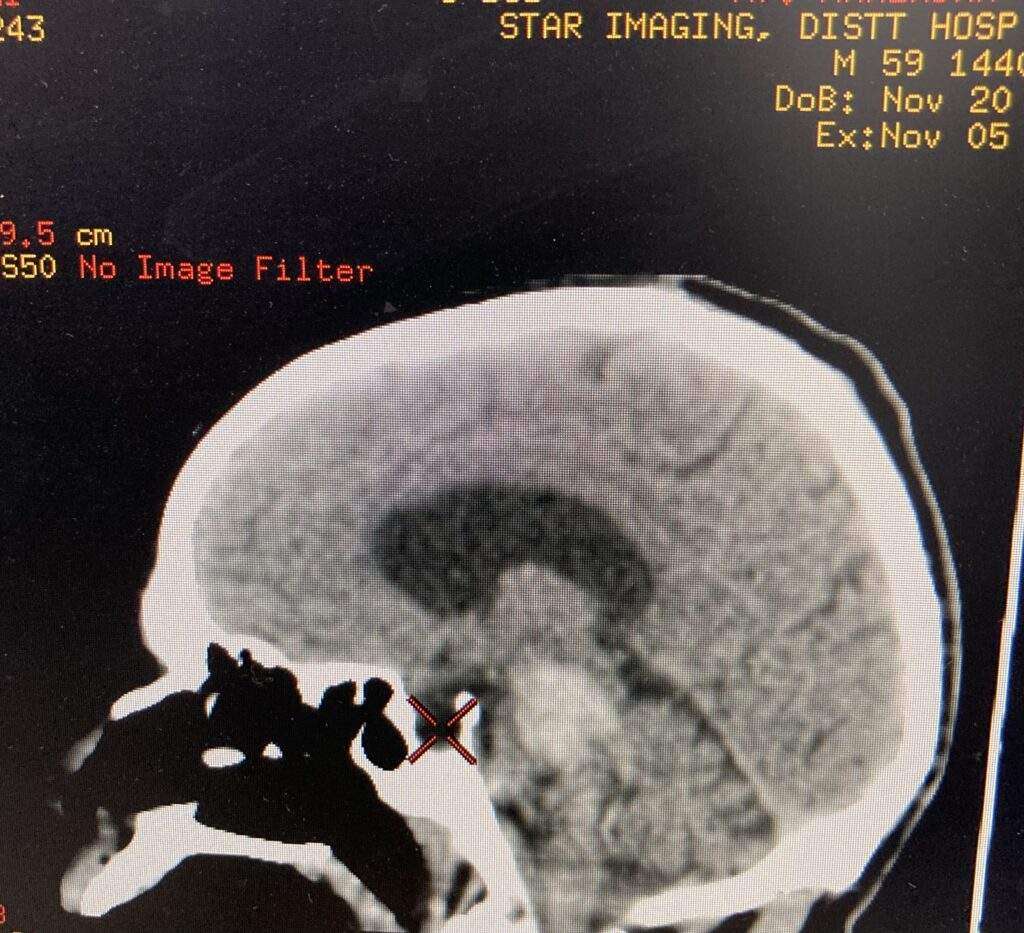
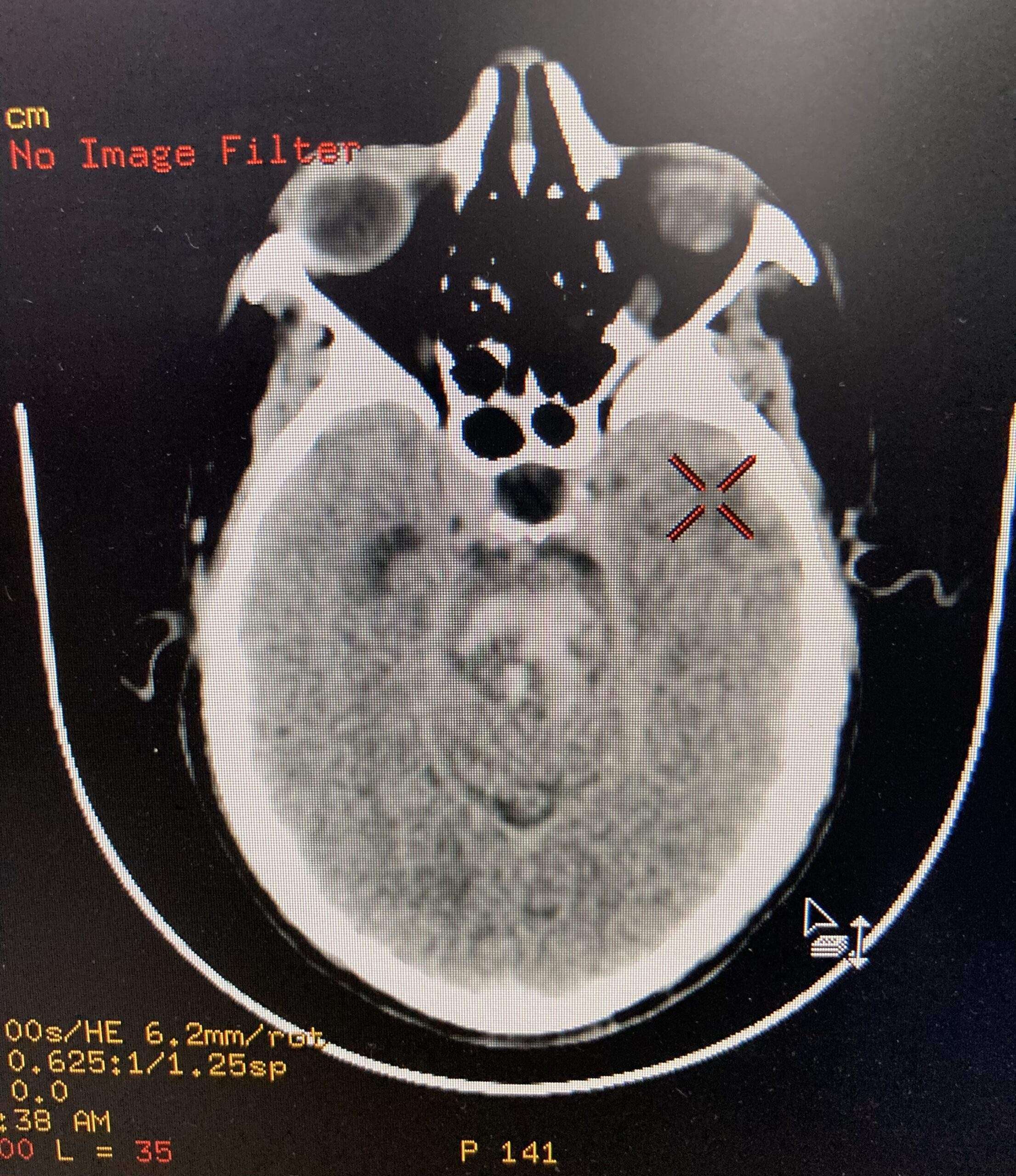
CT of the brain is usually the first, and often the only, investigation obtained upon presentation. Features typical of an acute intraparenchymal hemorrhage are noted, usually located centrally within the pons (on account of the larger paramedian perforators usually being the site of bleeding).
The hematoma more frequently extends in a rostro-caudal direction along the traversing long tracts rather than laterally into the middle cerebellar peduncle. Usually the hematoma does not extend beyond the pontomedullary junction inferiorly and the inferior midbrain superiorly. These hematomas frequently rupture into the 4th ventricle.
Pontine HemorrhagePontine Hemorrhage
MRI
In patients who have small volume bleeds and who are thought to possibly have an underlying lesion, MRI may be of use (e.g. identification of a vascular malformation).
Treatment and Prognosis
Patient with this hemorrhages have a poor prognosis, with large bleeds being almost universally fatal. Open surgical evacuation of the clot is usually not performed, although stereotactic clot aspiration has been advocated by some.
In smaller hemorrhages, medical management and treatment of hydrocephalus with extraventricular drains may be life-saving, however, often with significant residual neurological deficits.
Overall mortality ranges between 30% and 90%, with the overall volume of the bleed and initial GCS being related to outcome.
Rehabilitation for Pontine Stroke Survivors
Rehabilitation can take many forms to address the unique secondary effects caused by a pontine stroke. Therapists will help you create a custom rehabilitation plan that addresses your unique goals to improve movement and/or sensation.
One major goal of rehabilitation is to spark neuroplasticity to help rewire the brain and recover as much function as possible. Neuroplasticity is activated through massed practice as the brain gets better at the activities and skills that we repeatedly practice.
Here are some of types of therapy that are commonly used to treat the effects of a pontine stroke:
Physical Therapy
During physical therapy, your therapist will guide you through rehabilitation exercises that help improve mobility in the affected muscles. Survivors with severe motor impairments can start slow with passive range of motion exercises to help prevent complications such as contractures or pressure sores. Passive movement also helps spark neuroplasticity and rewire the brain. Over time, they may be able to progress to more active exercises and even strengthening.
Occupational Therapy
Your occupational therapist specializes in maximizing independence with the activities of daily living. Your OT will provide you with both functional exercises and any necessary compensation techniques to help you complete your daily tasks. They can also offer recommendations for home modifications to help prevent falls, discuss safety concerns and precautions following sensation loss, and provide resources for getting back to work or back to drive again.
Speech Therapy
Speech therapists are able to address difficulties with speaking, swallowing, and general communication skills. They may use a variety of exercises to improve the strength and coordination of the muscles surrounding your mouth and face. They can also suggest methods of communication other than speaking, called augmentative and alternative communication (AAC). For example, if you have locked-in syndrome, they may recommend using technology designed to track your eye movements to communicate.
Home Therapy
A strong home exercise program after stroke can make a noticeable difference during recovery. Whether you have mild, moderate, or severe effects that you wish to recover, your therapist can provide suitable exercises for you to practice at home. Home therapy is essential to keep the brain constantly stimulated and maximize neuroplasticity.
Sensory Retraining
Sometimes a pontine stroke can cause changes in sensation such as numbness, tingling, or difficulty sensing temperature. For these sensory issues, sensory retraining exercises might be able to help. It involves safely exposing your skin to various textures and temperatures to stimulate the brain.
Recovery from Pontine Stroke
Overall, a pontine stroke can affect movement and/or sensation on one or both sides of the body. Although pontine infarcts are technically small in nature, they can create significant effects such as locked-in syndrome, especially when both sides of the pons were affected.
Fortunately, with a rigorous rehabilitation regimen, survivors can stimulate the brain and maximize their chances of recovery. Not all survivors will achieve a full recovery, but it’s a possibility for many. Approach your stroke recovery prognosis with curiosity to see how far you can go.
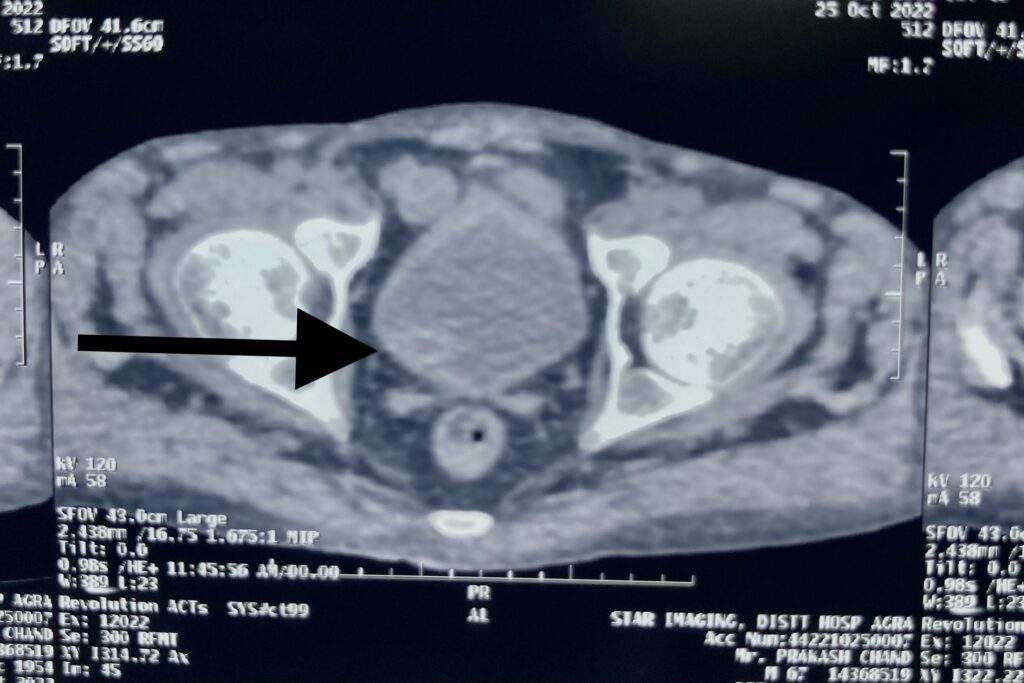
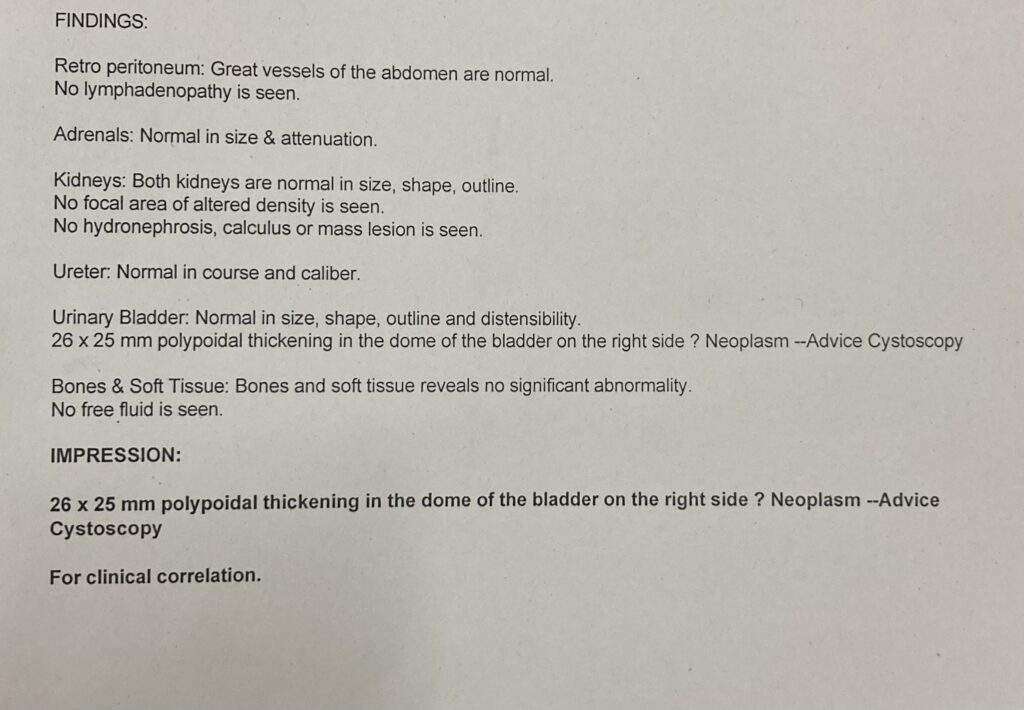
Urinary Bladder cancer is a common type of cancer that begins in the cells of the bladder. The bladder is a hollow muscular organ in your lower abdomen that stores urine.
Urinary bladder cancer most often begins in the cells (urothelial cells) that line the inside of your bladder. Urothelial cells are also found in your kidneys and the tubes (ureters) that connect the kidneys to the bladder. Urothelial cancer can happen in the kidneys and ureters, too, but it’s much more common in the bladder.
Most bladder cancers are diagnosed at an early stage, when the cancer is highly treatable. But even early-stage bladder cancers can come back after successful treatment. For this reason, people with bladder cancer typically need follow-up tests for years after treatment to look for bladder cancer that recurs.
What are Urinary bladder Cancer types?
There are three types of urinary bladder cancer. Each type is named for the cells that line the wall of your bladder where the cancer started. Bladder cancer types include:
Transitional cell carcinoma: This cancer starts in transitional cells in the inner lining of your bladder wall. About 90% of all bladder cancers are transitional. In this cancer type, abnormal cells spread from the inner lining to other layers deep in your bladder or through your bladder wall into fatty tissues that surround your bladder. This bladder cancer type is also known as urothelial bladder cancer.
Squamous cell carcinoma: Squamous cells are thin, flat cells that line the inside of your bladder. This bladder cancer accounts for about 5% of bladder cancers and typically develops in people who’ve had long bouts of bladder inflammation or irritation.
Adenocarcinoma: Adenocarcinoma cancers are cancers in the glands that line your organs, including your bladder. This is a very rare type of bladder cancer, accounting for 1% to 2% of all bladder cancers.
Small cell carcinoma of the bladder: This extremely rare type of bladder cancer affects about 1,000 people in the U.S.
Sarcoma: Rarely, soft tissue sarcomas start in bladder muscle cells.
Healthcare providers may also categorize bladder cancer as being noninvasive, non-muscle-invasive or muscle-invasive.
Noninvasive: This bladder cancer may be tumors in a small section of tissue or cancer that’s only on or near the surface of your bladder.
Non-muscle-invasive:This refers to bladder cancer that’s moved deeper into your bladder but hasn’t spread to muscle.
Muscle-invasive:This bladder cancer has grown into bladder wall muscle and may have spread into the fatty layers or tissues on organs outside of your bladder.
Risk Factors for Urinary Bladder Cancer
Cigarette smoke: Smoking cigarettes more than doubles your risk of developing bladder cancer. Smoking pipes and cigars and being exposed to second-hand smoke may also increase your risk.
Radiation exposure: Radiation therapy to treat cancer may increase your risk of developing bladder cancer.
Chemotherapy: Certain chemotherapy drugs may increase your risk.
Exposure to certain chemicals: Studies show that people who work with certain chemicals used in dyes, rubber, leather, paint, some textiles and hairdressing supplies may have an increased risk.
Frequent bladder infections: People who have frequent bladder infections, bladder stones or other urinary tract infections may be at an increased risk of squamous cell carcinoma.
Chronic catheter use: People who have a chronic need for a catheter in their bladder may be at risk for squamous cell carcinoma.
Symptoms of Urinary Bladder Cancer
Bladder cancer signs and symptoms may include:
Blood in urine (hematuria), which is painless and may cause urine to appear bright red or cola colored, though sometimes the urine appears normal and blood is detected on a lab test
Frequent urination
Painful urination
Back pain
Diagnosis of Urinary Bladder Cancer
Urinalysis: Providers use a variety of tests to analyze your pee. In this case, they may do urinalysis to rule out infection.
Cytology: Providers examine cells under a microscope for signs of cancer.
Cystoscopy: This is the primary test to identify and diagnose bladder cancer. For this test, providers use a pencil-sized lighted tube called a cystoscope to view the inside of your bladder and urethra. They may use a fluorescent dye and a special blue light that makes it easier to see cancer in your bladder. Providers may also take tissue samples while doing cystoscopies.
If urinalysis, cytology and cystoscopy results show you have bladder cancer, healthcare providers then do tests to learn more about the cancer, including:
Transurethral Resection of Bladder Tumor (TURBT): Providers do this procedure to remove bladder tumors for additional tests. TURBT procedures may also be a treatment, removing bladder tumors before the tumors can invade your bladder’s muscle wall. This test is an outpatient procedure done under spinal or general anesthesia.
Magnetic Resonance Imaging (MRI): This imaging test uses a magnet, radio waves and a computer to take detailed images of your bladder.
Computed Tomography (CT) Scan: Providers may do this test to see if cancer has spread outside of your bladder.
Chest X-ray: This test lets providers check for signs bladder cancer has spread to your lungs.
Bone scan: Like a chest X-ray, bone scans check for signs bladder cancer has spread to your bones.
Biopsies to look for cancer spread.
How do I take care of myself?
About half of all people with bladder cancer have early-stage cancer that’s relatively easy to treat. But bladder cancer often comes back (recurs). People who’ve had bladder cancer will need regular checkups after treatment. Being vigilant about follow-up care is one thing you can do to take care of yourself. Here are some other suggestions from the Bladder Cancer Advocacy Network include:
Follow a heart-healthy diet: Plan menus that include skinless poultry and fish, low-fat dairy products, nuts and legumes, and a variety of fruits and vegetables.
Focus on high-fiber foods: Bladder cancer treatment may cause digestive issues and a fiber-rich diet may help.
Get some exercise: Gentle exercise may help manage stress.
Connect with others: Bladder cancer often comes back. It’s not easy to have a rare disease that’s likely to return. Connecting with people who understand what you’re going through may help.
If you have bladder cancer, it may help to know about half of all people with the condition receive treatment when their tumors are limited to the inner layer of their bladder wall. For them, surgery to remove tumors means they’re cancer-free. But bladder cancer often comes back (recurs). If you’re worried about recurring cancer, talk to your healthcare provider. They’re your best resource for information on risk factors that increase the chance you’ll have another bout of bladder cancer. They’ll help you stay vigilant about symptoms that may be signs of recurring bladder cancer and be there for you if you need more bladder cancer treatment.
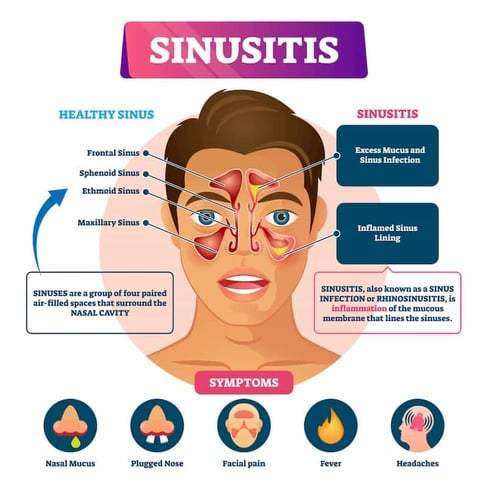
An infection of the sinuses is known as acute sinusitis. Rhinosinusitis is often a better word since the sinus passageways and nasal passages are connected. Acute rhinosinusitis is a frequent diagnosis, resulting in a significant amount of yearly healthcare costs and plenty of visits to primary care facilities. Additionally, it is a typical justification for prescribing antibiotics.
It can be brought on by bacterial, viral, or fungal infections, with viral infections being the most frequent. Antibiotics are frequently overprescribed in the treatment of this ailment, so it’s crucial to understand how to correctly examine a sinusitis patient and determine when antibiotics are necessary. In accordance with the recommendations made by several societies, this article covers the causes of rhinosinusitis and when antibiotic treatment in the management of this illness might be appropriate.
Different types of rhinosinusitis may be separated into the following categories based on consensus opinions :
Acute – Signs and symptoms for fewer than four weeks.
Subacute – It takes between four and twelve weeks for symptoms to subside.
Chronic – Enduring symptoms for more than 12 weeks.
Recurrent – Four episodes lasting fewer than four weeks, with full symptom relief between each episode.
Occurrence
One out of every five antibiotic prescriptions for adults is for acute rhinosinusitis, making it the sixth most prevalent cause for an antibiotic prescription. 6 to 7 per cent of children with respiratory symptoms are affected by acute rhinosinusitis.
Approximately,
16% of individuals are diagnosed yearly with ABRS. Given the clinical nature of this diagnosis, an overestimation is possible.
An estimated 0.5 to 2.0% of viral rhinosinusitis (VRS) in adults.
And 5 to 10% of children will progress to bacterial infections.
Causes
The most prevalent cause of acute rhinosinusitis is viruses.
The microorganisms responsible for viral rhinosinusitis (VRS) include rhinovirus, adenovirus, influenza virus, and parainfluenza virus.
Streptococcus pneumonia (38%) is the most prevalent cause of acute bacterial rhinosinusitis (ABRS), followed by Haemophilus influenzae (36%) and Moraxella catarrhalis (16%).
Rarely, fungal infections may also cause acute rhinosinusitis, although this is virtually only seen in immunocompromised people.
It is crucial to distinguish between acute invasive fungal sinusitis (IFS) and allergic fungal sinusitis (AFS), which manifests in immunocompetent people as a mass-like lesion filling a sinus canal and often causes persistent symptoms.
How to assess the patient?
1. Clinical evaluations often identify acute rhinosinusitis. The most sensitive and specific “cardinal” symptoms for acute rhinosinusitis are purulent nasal discharge accompanied by nasal obstruction or face pain/pressure/fullness. This must be determined particularly from people who report “headache” as a general complaint. Facial pressure is a symptom of sinusitis, but the headache is not (with the rare exception of sphenoid sinusitis, which may manifest as an occipital or vertex headache and is often persistent). The observant doctor must gather this information from the patient in order to ascertain the patient’s precise symptoms.
2. ABRS may be diagnosed if cardinal symptoms continue beyond ten days or if they intensify after an initial period of recovery (“double worsening”). Acute rhinosinusitis is accompanied by cough, weariness, hyposmia, anosmia, maxillary dental discomfort, and ear fullness or pressure. Mucopus coming from the osteomeatal complex may be detected by anterior rhinoscopy, or it may be proven by formal endoscopic rhinoscopy in the clinic.
3. The clinical manifestation of ABRS differs somewhat across children. Children are more likely to appear with fevers, in addition to the 10-day length, cardinal symptoms, and “double worsening.” Initial nasal discharge may be watery, then become purulent. Approximately 80% of acute bacterial sinusitis is preceded by an upper respiratory infection.
4. The severity of the symptoms suggests a bacterial origin. At the onset of the disease, these symptoms include high fevers (above 39 C or 102 F) accompanied by purulent nasal discharge or face discomfort for three to four consecutive days. Generally, viral diseases resolve within three to five days.
Antibiotic resistance issues must also be taken into account. These include:
Antibiotic usage during the past month
Hospitalisation within the preceding five days
Healthcare profession
Local antibiotic resistance trends are known to local healthcare providers
Finally, it is important to determine whether a patient is at increased risk. Included among these attributes are:
Comorbidities (i.e., cardiac, renal, or hepatic disease)
Immunocompromised states
Age under 2 years or over 65 years
5. In immunocompromised patients, acute fungal rhinosinusitis is often accompanied by fevers, nasal blockage or bleeding, and face discomfort; however, it may also be asymptomatic. Refractory or severe symptoms should urge investigation of this diagnosis in immunocompromised patients.
How to diagnose the condition?
Clinical evaluations often identify acute rhinosinusitis. It is essential for the doctor to differentiate between VRS and ABRS in order to guarantee the appropriate use of antibiotics.
Local resistance patterns and prevalence of penicillin non-susceptible S. pneumoniae warrants clarification.
The conventional diagnostic criteria for adult rhinosinusitis include the presence of at least two significant symptoms or one major symptom plus two or more mild symptoms. In youngsters, the requirements are the same, with the exception of a greater focus on nasal discharge (rather than nasal obstruction).
Principal Symptoms :
Purulent anterior nasal discharge
Fever (for acute sinusitis only)
Purulent or discoloured posterior nasal discharge
Facial congestion or fullness
Nasal congestion or obstruction
Facial pain or pressure
Hyposmia or anosmia
Mild features:
Headache
Ear pain or pressure or fullness
Halitosis
Dental pain
Cough
Fever (for subacute or chronic sinusitis)
Fatigue
Here is some clinical advice for telling ABRS from VRS:
Duration of symptoms exceeding 10 days.
At the onset of the disease, a high temperature (above 39 C or 102 F) is accompanied by purulent nasal discharge or face discomfort for three to four consecutive days.
Increase in symptom severity within the first 10 days.
In general, routine laboratory testing is unnecessary. Evaluations for cystic fibrosis, ciliary dysfunction, and immunodeficiency should be considered for chronic, recurring, or persistent rhinosinusitis. Some data suggest that a high ESR and CRP may indicate a bacterial infection.
The gold standard is the culture of endoscopic aspirates with more than or equal to 10 CFU/mL. However, this is not required for ABRS diagnosis and is not performed in the great majority of instances. Due to their weak connection with endoscopic aspirates, nasal and nasopharyngeal cultures are of little value. Referral for endoscopic aspiration may be beneficial for individuals with resistant infections or numerous antibiotic sensitivities.
Imaging is rarely indicated for acute sinusitis unless there is clinical concern for a complication or alternate diagnosis. Plain sinus films are often ineffective in identifying inflammation. They may display air-fluid levels. However, this does not aid in distinguishing between viral and bacterial etiologies. If a complication or other diagnosis is suspected, or if the patient has repeated acute infections, sinus CT imaging should be performed to evaluate for bone, soft tissue, dental, or other structural abnormalities, as well as chronic sinusitis.
These should be attained after an acceptable course of therapy. CT scans of the sinuses may reveal air-fluid levels, opacification, and inflammation. Over 5 mm of thicker sinus mucosa is symptomatic of inflammation. Additionally, it can efficiently evaluate bone deterioration or disintegration. However, these data are not useful for distinguishing between viral and bacterial etiologies.
MRI provides more information than sinus CT when evaluating soft tissue or illuminating a malignancy. Consequently, MRI may be useful for determining the severity of problems in situations involving ocular or cerebral extension.
How to manage the condition?
Antibiotic medication or a period of cautious waiting may be used to treat ABRS, provided that reliable follow-up is assured. There are minor differences in the guidelines of various expert committees.
The amended 2015 American Academy of Otolaryngology Adult Sinusitis guideline suggests amoxicillin with or without clavulanate for 5 to 10 days as first-line treatment for the majority of people. Failure of treatment is determined if symptoms do not improve or worsen within seven days.
The Infectious Disease Society of America Guidelines for Acute Bacterial Rhinosinusitis prescribe amoxicillin with clavulanate for 10 to 14 days in children and 5 to 7 days in adults as first-line treatment. Failure of treatment is determined if symptoms do not improve within 3 to 5 days or worsen within 48 to 72 hours.
theAmerican Academy of Pediatrics Clinic Practice Guideline for the diagnosis and management of acute bacterial sinusitis in children aged 18 years recommended amoxicillin with or without clavulanate as first-line treatment. Uncertainty surrounds the length of therapy, although their recommendation was to continue treatment for a further seven days after symptoms disappear.
If, after 72 hours of therapy, symptoms do not improve or worsen, the treatment has failed. If the patient cannot accept oral fluids, ceftriaxone 50 mg/kg may be administered. If the patient can tolerate oral fluids the next day and improves, he or she may then begin an oral antibiotic regimen. To effectively address beta-lactamase-producing bacteria, a separate article recommends amoxicillin with clavulanate as the first treatment for children.
Adding clavulanate or prescribing high-dose amoxicillin (90mg/kg/day vs 45mg/kg/day) in children is determined by local antibiotic resistance trends, the patient’s risk level, risk factors for antibiotic resistance, and the severity of symptoms.
A third-generation cephalosporin with clindamycin (for enough coverage of non-susceptible S. pneumoniae) or doxycycline might be therapeutic options for penicillin-allergic individuals. The effectiveness of third-generation cephalosporins alone against S. pneumoniae is inconsistent. Fluoroquinolones might also be explored, although they have a greater incidence of adverse effects. In youngsters, doxycycline and fluoroquinolones should be administered with more care. S. pneumoniae and Hemophilus influenzae have elevated levels of resistance to second-generation cephalosporins, trimethoprim/sulfamethoxazole, and macrolides.
There is also evidence that antibiotic medication does not always reduce the duration of symptoms or the risk of complications in adults. Many instances of ABRS may also resolve spontaneously within two weeks.
Symptomatic therapies
Clinicians may give symptomatic therapies, but generally, there is a lack of conclusive data. In guidelines, nasal steroids and nasal saline irrigation are the most popular suggestions. By lowering mucosal oedema, intranasal steroids may assist in relieving the blockage. A limited number of clinical studies suggested that greater dosages of intranasal corticosteroids may reduce the period of symptom remission by two to three weeks. Additionally, nasal saline irrigation may aid in reducing blockage. Due to their ability to thicken nasal secretions, antihistamines are not recommended unless there is a definite allergic component.
Be aware of potential complications
Complications are uncommon, occurring in around one out of every thousand cases. Infections of the sinuses may extend to the orbit, bone, and cerebral cavities. 80% of orbitocranial problems manifest in the orbit. These problems may be associated with substantial morbidity and death. Due to the very thin ethmoid bone that divides infections from the ethmoid from the orbit, the orbit is the most likely location.
Prognosis
Most cases of acute bacterial rhinosinusitis are viral. The vast majority of cases are either self-limiting or efficiently treatable with antibiotics. In immunocompromised individuals, invasive fungal rhinosinusitis is an uncommon but severe type of illness. It is related to a high risk of morbidity and death.
It is a viral infection that causes an outbreak of a painful rash or blisters on the skin. It’s caused by the varicella-zoster virus, which is the same virus that causes chickenpox. The rash most often appears as a band of rashes or blisters in one area of your body.
Where does it come from?
When you have chickenpox as a child, your body fights off the varicella-zoster virus and the physical signs of chickenpox fade away, but the virus always remains in your body. In adulthood, sometimes the virus becomes active again. This time, the varicella-zoster virus makes its second appearance in the form of shingles.
How common is shingles?
About 1 million cases are diagnosed every year. The risk of shingles increases as you get older, with about half the cases occurring in people over the age of 50. Shingles develops in about 10% of people who have had chickenpox at an earlier time in their lives.
Who is at risk for getting shingles?
People who have had chickenpox who are more likely to develop shingles include those:
With a weakened immune system (such as people with cancer, HIV, organ transplant recipients or those receiving chemotherapy).
Over the age of 50.
Who have been ill.
Who have experienced trauma.
Who are under stress.
The chickenpox virus doesn’t leave your body after you have chickenpox. Instead, the virus stays in a portion of your spinal nerve root called the dorsal root ganglion. For the majority of people, the virus stays there quietly and doesn’t cause problems. Researchers aren’t always sure why the virus gets reactivated, but this typically occurs at times of stress.
Can you get shingles more than once?
Yes, you can get shingles more than one time. One of the biggest myths about shingles is that it can only happen once. This isn’t true. You can have more than one episode. If you get shingles again, you usually don’t get the rash in the same place.
What are the symptoms?
Early symptoms may include:
Fever.
Chills.
Headache.
Feeling tired.
Sensitivity to light.
Stomach upset.
Other signs and symptoms that appear a few days after the early symptoms include:
An itching, tingling or burning feeling in an area of your skin.
Redness on your skin in the affected area.
Raised rash in a small area of your skin.
Fluid-filled blisters that break open then scab over.
Mild to severe pain in the area of skin affected.
How long does a shingles outbreak last?
It can take three to five weeks from the time you begin to feel symptoms until the rash totally disappears.
First, a few days before the rash appears, you may feel pain in an area on your skin. The pain is described as itching, burning, stabbing or shooting. This usually happens before the rash comes.
Next, the raised rash appears as a band or a patch, usually on one side of your body. The rash usually appears around your waistline or on one side of your face, neck, or on the trunk (chest/abdomen/back), but not always. It can occur in other areas including your arms and legs.
Within three to four days, the rash develops into red, fluid-filled, painful, open blisters.
Usually, these blisters begin to dry out and crust over within about 10 days.
The scabs clear up about two to three weeks later.
Do you always get the typical rash if you have shingles?
Occasionally, some people don’t get a rash. If you have any of the other symptoms (even without a rash), see your healthcare provider sooner rather than later. There are effective treatments you can take early for shingles. Even if you don’t have shingles, seeing your healthcare provider will help you get your condition diagnosed and treated.
Why does shingles appear mostly on one side or in one area of your body?
The virus travels in specific nerves, so you will often see shingles occur in a band on one side of your body. This band corresponds to the area where the nerve transmits signals. These rash stays somewhat localized to an area. It doesn’t spread over your whole body. Your torso is a common area, as is your face.
Is shingles contagious?
Someone can’t spread shingles to another person, but they can spread chickenpox. The varicella-zoster virus is spread through direct skin-to-skin contact with the fluid that oozes from the blisters. Shingles is rarely spread by breathing in the varicella-zoster virus the way airborne viruses are spread. If your rash is in the blister phase, stay away from those who haven’t had chickenpox or the chickenpox vaccine and keep your rash covered.
How long are you contagious if you have shingles?
If you have such lesion, you’re contagious until the rash is dried and crusted over. The varicella-zoster virus can only cause chickenpox in someone who has never had chickenpox or hasn’t been vaccinated against chickenpox.
How is shingles diagnosed?
It can be diagnosed by the way the rash is distributed on your body. The blisters of a shingles rash usually appear in a band on one side of your body. It may also be diagnosed in a laboratory using scrapings or a swab of the fluid from the blisters.
How is shingles treated?
There is no cure for shingles but there are treatments for managing the symptoms.
Antiviral medications
These drugs may ease the discomfort and make the symptoms stop sooner, particularly if you start them within 72 hours of the first sign of shingles. They may also help prevent the pain that can happen months and years later, called post-herpetic neuralgia. These medications include:
Acyclovir.
Famciclovir.
Valacyclovir.
Over-the-counter pain medications
These medications include the following and may be effective in relieving pain:
Acetaminophen.
Ibuprofen.
Other medications
Antibacterial drugs may be prescribed if you develop a bacterial infection due to the shingles rash. Anti-inflammatory drugs like prednisone may be prescribed if shingles affects your eyes or other parts of your face.
If you have more than one area of blisters, what can you expect if you go to the hospital?
It’s important to note that most people with shingles don’t need to be in a hospital, but if you do:
You’ll be in a contact isolation room.
The door will be kept closed.
A sign on your door will remind people who have never had chickenpox or the vaccine not to enter.
The sign will also remind staff to wear gowns and gloves when entering the room.
If you have shingles in only one area of your body that can’t be kept covered, what can you expect for your hospital stay?
You will be in a contact isolation room.
The sign on the door will remind staff to wear gowns and gloves when entering the room.
What are the complications of shingles?
After the shingles rash has disappeared, you might continue to have nerve pain in that same area. Post-herpetic neuralgia can last for months or years and become quite severe.
More than 10% of people who get shingles develop post-herpetic neuralgia. Researchers don’t know why some people get post-herpetic neuralgia and others don’t. It may be that nerves become more sensitive or that the virus may be invading and damaging the central nervous system.
Other complications include:
Other types of nerve issues like numbness or itching.
A bacterial infection of the shingles rash.
Eye and ear inflammation if the rash is near these organs.
Is shingles dangerous or even fatal?
If shingles involves your eye, it can lead to blindness. In rare cases, shingles can lead to hearing problems, pneumonia, inflammation of the brain (encephalitis) and even death.
How is post-herpetic neuralgia treated?
Treatments include lotions or creams (such as lidocaine or capsaicin) and/or other medications not specifically used for pain, such as antidepressants or drugs for epilepsy. Regular pain relievers are not usually effective for this type of pain.
If your pain doesn’t lessen, you might try therapies like nerve blocks or steroid injections near the area where the nerves exit the spine. Your provider might suggest an implantable nerve stimulator device for severe, ongoing pain that hasn’t responded to other treatments.
Is a vaccine available to prevent shingles?
Two vaccines are available in the market to reduce your chance of developing shingles and post-herpetic neuralgia. One vaccine, Zostavax®, has been available since 2006. The second vaccine, Shingrix®, has been available since 2017. Shingrix is recommended as the preferred vaccine by the Advisory Committee on Immunization Practices, a group of medical and public health experts.
Shingrix (recombinant zoster vaccine) is given as a two-dose shot in your upper arm. You should receive the second dose (shot) two to six months after receiving the first. Shingrix has been shown to be more than 90% effective in preventing shingles and postherpetic neuralgia. Its effectiveness remains above 85% for at least four years after receiving the vaccine.
Who should be vaccinated with Shingrix?
The Shingrix vaccine is recommended for those 50 years of age and older who are in good health.
You should get the Shingrix vaccine even if:
You’ve had shingles already.
You’ve been previously vaccinated with Zostavax (a live zoster vaccine). If you’ve been vaccinated with Zostavax, wait at least eight weeks before getting vaccinated with Shingrix.
You don’t know for sure if you’ve ever had chickenpox.
Ask your healthcare provider, who knows your entire health history if getting this vaccine is right for you.
Who should not be vaccinated with Shingrix?
You shouldn’t receive the Shingrix vaccine if you:
Have ever had a severe allergy to this vaccine or any ingredient in this vaccine.
Are breastfeeding or pregnant.
Currently have shingles.
Are ill and have a high fever.
Have tested negative for immunity to varicella-zoster virus (get the chickenpox vaccine instead).
Ask your healthcare provider if the benefits of getting the vaccine outweigh any potential risks.
What serious side effects should you watch for after getting the Shingrix vaccine?
Serious side effects from vaccines are extremely rare. However, call or go to the nearest emergency room right away if you experience any of the following within minutes to hours after receiving Shingrix:
Swelling of your face or throat.
Difficulty breathing.
Hives.
Fast heartbeat.
Dizziness, lightheadedness, weakness.
If you’ve had shingles recently, how long should you wait before getting the Shingrix vaccine?
You can get the Shingrix vaccine any time after the shingles rash has gone away.
When is it safe to return to work if you have shingles?
You can return to work when you feel well enough to return and you’re no longer contagious. This means that your blistered rash has dried up and scabbed over. This usually takes up to 10 days from the time the rash first appears.
Are there natural ways to boost your immune system to help lessen the chances of developing shingles?
Stress is a risk factor for developing it, so limiting your stress can be helpful. Try meditation, yoga or other relaxation methods.
Other things you can do include:
Eat a healthy diet.
Maintain a healthy weight.
Exercise regularly.
Aim for seven to nine hours of sleep each night.
Don’t smoke or use tobacco products.
These are all tips for an overall healthy lifestyle, not just for reducing your chance of getting shingles.
What is the difference between herpes zoster and varicella-zoster?
Herpes zoster is simply another medical name for shingles. Varicella-zoster is the virus that causes both shingles and chickenpox.
If you’ve had chickenpox, you’re at risk of developing shingles later in life. It causes a rash that is contagious and painful. The disease can have serious complications. The best thing you can do to reduce your risk is to get the shingles vaccine. The vaccines are safe and effective.
A urinary catheter is a medical device made from a thin, hollow tube that can be inserted through the urethra or through a small opening in the abdomen, in order to drain urine from the bladder. Male external catheters, though they share a similar name, are shaped like a condom and are designed to slip over the penis rather than being inserted into the body.
How does a urinary catheter work?
The hollow tube has openings at the end, so that when it is inserted into the bladder, the urine will naturally flow out through the tube into a collection bag or the toilet. Male external catheters have an adhesive that creates a leak-proof seal around the penis with an opening at the end so the urine will flow out the front, through a tube and into a collection bag.
How is the urinary catheter inserted?
Indwelling catheters will be inserted by a medical professional through the urethra or though a small opening in the abdomen in the case of suprapubic catheters. Intermittent catheters are inserted into the urethra and this can be done by yourself at home, or by a nurse or caregiver.
How do urinary catheters stay in?
Once an indwelling catheter is inserted into the bladder, an area near the end of the catheter can be inflated with sterile water, like a balloon. This small balloon is much bigger than the urethra so it holds the catheter in place, preventing it from slipping out and still allowing urine to drain through the tube in the middle of the balloon. The balloon can be deflated when the catheter is removed. Keep in mind, not all catheters stay in. Intermittent catheters are inserted only when the bladder is full, quickly draining the bladder and then removed when the bladder has emptied.
Why are urinary catheters used?
There are a great variety of diagnoses that would result in the need of a catheter. Sometimes a catheter is needed only temporarily during hospitalization. Often times they are used permanently when the bladder does not function normally or when the bladder cannot be controlled. Catheters may be used as a solution for bladder retention (inability to empty the bladder) or bladder incontinence (inability to control the bladder).
There are three main types of catheters: indwelling catheters, intermittent catheters, and external catheters for men. Catheters come in different materials, with differently shaped tips based on the user’s needs. More information on the types of catheters can be found below.
Indwelling urinary catheters
Indwelling catheters are designed to be inserted through the urethra (Foley catheter) or a small opening in the abdomen (suprapubic catheter). Indwelling catheters are designed to stay inside the body to continuously drain the bladder. Indwelling catheters are inserted by a medical professional and can be used long term, with the catheter being changed monthly.
Intermittent urinary catheters
Intermittent catheters are also known as “in and out” catheters because they are inserted and removed around 5 times a day. When inserted, they are designed to drain the bladder all at once and then be removed. The insertion of an intermittent catheter can be done in the home once the user learns the technique and has had a little practice. There are different variations of intermittent catheters, explained below.
Straight intermittent catheter: This catheter can be made from latex or silicone, is generally used with lubricant, and has a funnel at the end to drain into the toilet. This is the standard intermittent catheter.
Closed system catheters: These come pre-lubricated and are attached to a collection bag. The system is sterile and touch-free, which can help prevent infections. The urine drains into the collection bag and then is disposed of, allowing for convenient catheterization when there is not a restroom nearby.
Hydrophilic coated catheters: Catheters coated with a slippery surface that is activated with water. This eliminates the need for a separate lubricant and may reduce irritation to the urethra for frequent catheter users.
Male External Catheters, a.k.a. Condom Catheters
Male external catheters are also known as condom catheters, Texas catheters, or “gizmos.” These are different from the other catheters because they are external, so they are not inserted into the body. These catheters fit like a condom, so they can be slipped over the penis in the same way. Usually they will have an adhesive that seals against the skin of the penis, preventing leakage.
A tube connects to the front of the catheter, allowing the urine to flow out into a collection bag. Male external catheters are generally used for continuous draining of the bladder. They can be used at home with proper training, or a medical professional can change it for you. Male external catheters should be changed daily.
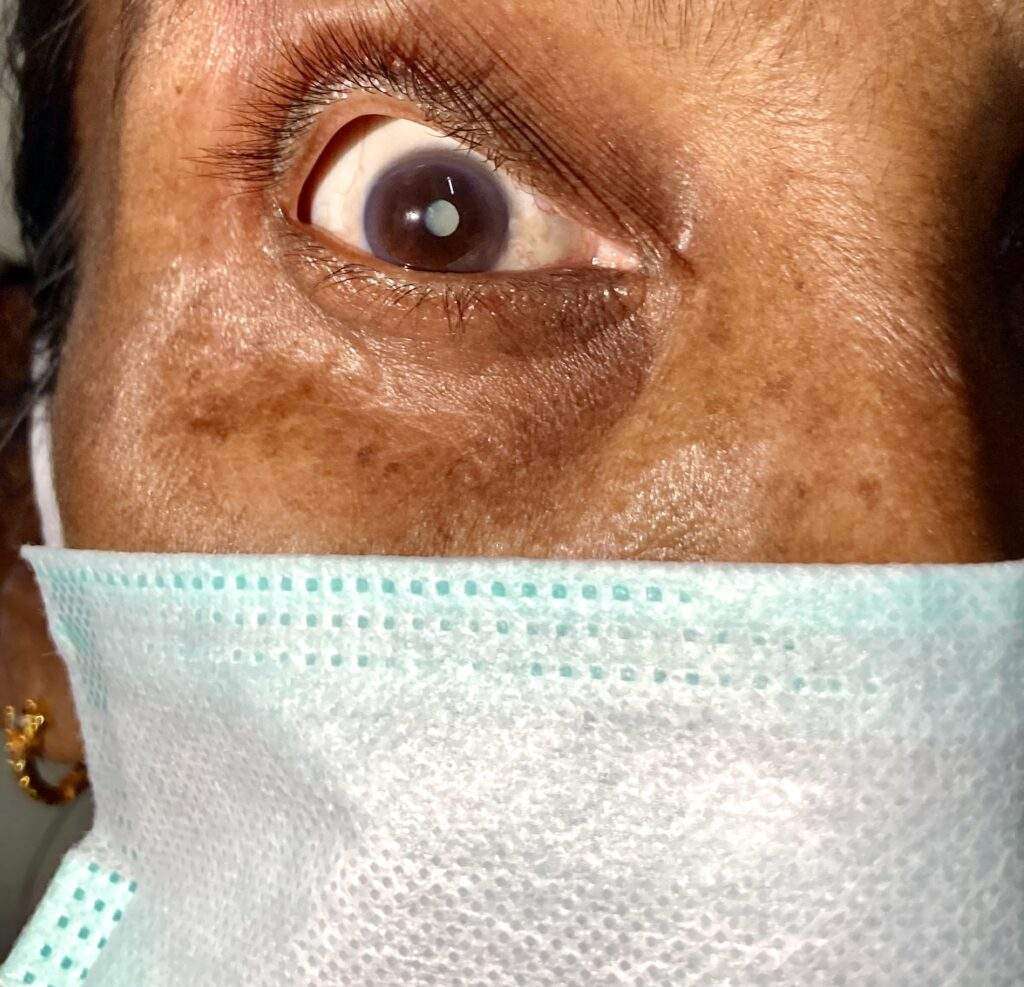
A cataract is a clouding of the normally clear lens of the eye. For people who have cataracts, seeing through cloudy lenses is a bit like looking through a frosty or fogged-up window. Clouded vision caused by cataracts can make it more difficult to read, drive a car (especially at night) or see the expression on a friend’s face.
Most cataracts develop slowly and don’t disturb your eyesight early on. But with time, cataracts will eventually interfere with your vision.
At first, stronger lighting and eyeglasses can help you deal with cataracts. But if impaired vision interferes with your usual activities, you might need cataract surgery. Fortunately, cataract surgery is generally a safe, effective procedure.
Symptoms
Signs and symptoms of cataracts include:
Clouded, blurred or dim vision
Increasing difficulty with vision at night
Sensitivity to light and glare
Need for brighter light for reading and other activities
Seeing “halos” around lights
Frequent changes in eyeglass or contact lens prescription
Fading or yellowing of colors
Double vision in a single eye
Cataract in 62 year old OPD Patient
At first, the cloudiness in your vision caused by a cataract may affect only a small part of the eye’s lens and you may be unaware of any vision loss. As the cataract grows larger, it clouds more of your lens and distorts the light passing through the lens. This may lead to more-noticeable symptoms.
When to see a doctor
Make an appointment for an eye exam if you notice any changes in your vision. If you develop sudden vision changes, such as double vision or flashes of light, sudden eye pain, or sudden headache, see your doctor right away.
Causes
Most cataracts develop when aging or injury changes the tissue that makes up the eye’s lens. Proteins and fibers in the lens begin to break down, causing vision to become hazy or cloudy.
Some inherited genetic disorders that cause other health problems can increase your risk of cataracts. Cataracts can also be caused by other eye conditions, past eye surgery or medical conditions such as diabetes. Long-term use of steroid medications, too, can cause cataracts to develop.
How a cataract forms
A cataract is a cloudy lens. The lens is positioned behind the colored part of your eye (iris). The lens focuses light that passes into your eye, producing clear, sharp images on the retina — the light-sensitive membrane in the eye that functions like the film in a camera.
As you age, the lenses in your eyes become less flexible, less transparent and thicker. Age-related and other medical conditions cause proteins and fibers within the lenses to break down and clump together, clouding the lenses.
As the cataract continues to develop, the clouding becomes denser. A cataract scatters and blocks the light as it passes through the lens, preventing a sharply defined image from reaching your retina. As a result, your vision becomes blurred.
Cataracts generally develop in both eyes, but not always at the same rate. The cataract in one eye may be more advanced than the other, causing a difference in vision between eyes.
Types of cataracts
Cataract types include:
Cataracts affecting the center of the lens (nuclear cataracts). A nuclear cataract may at first cause more nearsightedness or even a temporary improvement in your reading vision. But with time, the lens gradually turns more densely yellow and further clouds your vision.As the cataract slowly progresses, the lens may even turn brown. Advanced yellowing or browning of the lens can lead to difficulty distinguishing between shades of color.
Cataracts that affect the edges of the lens (cortical cataracts). A cortical cataract begins as whitish, wedge-shaped opacities or streaks on the outer edge of the lens cortex. As it slowly progresses, the streaks extend to the center and interfere with light passing through the center of the lens.
Cataracts that affect the back of the lens (posterior subcapsular cataracts). A posterior subcapsular cataract starts as a small, opaque area that usually forms near the back of the lens, right in the path of light. A posterior subcapsular cataract often interferes with your reading vision, reduces your vision in bright light, and causes glare or halos around lights at night. These types of cataracts tend to progress faster than other types do.
Cataracts you’re born with (congenital cataracts). Some people are born with cataracts or develop them during childhood. These cataracts may be genetic, or associated with an intrauterine infection or trauma.These cataracts may also be due to certain conditions, such as myotonic dystrophy, galactosemia, neurofibromatosis type 2 or rubella. Congenital cataracts don’t always affect vision, but if they do, they’re usually removed soon after detection.
Risk factors
Factors that increase your risk of cataracts include:
Increasing age
Diabetes
Excessive exposure to sunlight
Smoking
Obesity
High blood pressure
Previous eye injury or inflammation
Previous eye surgery
Prolonged use of corticosteroid medications
Drinking excessive amounts of alcohol
Prevention
No studies have proved how to prevent cataracts or slow the progression of cataracts. But doctors think several strategies may be helpful, including:
Have regular eye examinations. Eye examinations can help detect cataracts and other eye problems at their earliest stages. Ask your doctor how often you should have an eye examination.
Quit smoking. Ask your doctor for suggestions about how to stop smoking. Medications, counseling and other strategies are available to help you.
Manage other health problems. Follow your treatment plan if you have diabetes or other medical conditions that can increase your risk of cataracts.
Choose a healthy diet that includes plenty of fruits and vegetables. Adding a variety of colorful fruits and vegetables to your diet ensures that you’re getting many vitamins and nutrients. Fruits and vegetables have many antioxidants, which help maintain the health of your eyes.Studies haven’t proved that antioxidants in pill form can prevent cataracts. But a large population study recently showed that a healthy diet rich in vitamins and minerals was associated with a reduced risk of developing cataracts. Fruits and vegetables have many proven health benefits and are a safe way to increase the amount of minerals and vitamins in your diet.
Wear sunglasses. Ultraviolet light from the sun may contribute to the development of cataracts. Wear sunglasses that block ultraviolet B (UVB) rays when you’re outdoors.
Reduce alcohol use. Excessive alcohol use can increase the risk of cataracts.
Diagnosis
To determine whether you have a cataract, your doctor will review your medical history and symptoms, and perform an eye examination. Your doctor may conduct several tests, including:
Visual acuity test. A visual acuity test uses an eye chart to measure how well you can read a series of letters. Your eyes are tested one at a time, while the other eye is covered. Using a chart or a viewing device with progressively smaller letters, your eye doctor determines if you have 20/20 vision or if your vision shows signs of impairment.
Slit-lamp examination. A slit lamp allows your eye doctor to see the structures at the front of your eye under magnification. The microscope is called a slit lamp because it uses an intense line of light, a slit, to illuminate your cornea, iris, lens, and the space between your iris and cornea. The slit allows your doctor to view these structures in small sections, which makes it easier to detect any tiny abnormalities.
Retinal exam. To prepare for a retinal exam, your eye doctor puts drops in your eyes to open your pupils wide (dilate). This makes it easier to examine the back of your eyes (retina). Using a slit lamp or a special device called an ophthalmoscope, your eye doctor can examine your lens for signs of a cataract.
Applanation tonometry. This test measures fluid pressure in your eye. There are multiple different devices available to do this.
Treatment
When your prescription glasses can’t clear your vision, the only effective treatment for cataracts is surgery.
When to consider cataract surgery
Talk with your eye doctor about whether surgery is right for you. Most eye doctors suggest considering cataract surgery when your cataracts begin to affect your quality of life or interfere with your ability to perform normal daily activities, such as reading or driving at night.
It’s up to you and your doctor to decide when cataract surgery is right for you. For most people, there is no rush to remove cataracts because they usually don’t harm the eyes. But cataracts can worsen faster in people with certain conditions, including diabetes, high blood pressure or obesity.
Delaying the procedure generally won’t affect how well your vision recovers if you later decide to have cataract surgery. Take time to consider the benefits and risks of cataract surgery with your doctor.
If you choose not to undergo cataract surgery now, your eye doctor may recommend periodic follow-up exams to see if your cataracts are progressing. How often you’ll see your eye doctor depends on your situation.
What happens during cataract surgery
Cataract surgery involves removing the clouded lens and replacing it with a clear artificial lens. The artificial lens, called an intraocular lens, is positioned in the same place as your natural lens. It remains a permanent part of your eye.
For some people, other eye problems prohibit the use of an artificial lens. In these situations, once the cataract is removed, vision may be corrected with eyeglasses or contact lenses.
Cataract surgery is generally done on an outpatient basis, which means you won’t need to stay in a hospital after the surgery. During cataract surgery, your eye doctor uses a local anesthetic to numb the area around your eye, but you usually stay awake during the procedure.
Cataract surgery is generally safe, but it carries a risk of infection and bleeding. Cataract surgery increases the risk of retinal detachment.
After the procedure, you’ll have some discomfort for a few days. Healing generally occurs within a few weeks.
If you need cataract surgery in both eyes, your doctor will schedule surgery to remove the cataract in the second eye after you’ve healed from the first surgery.
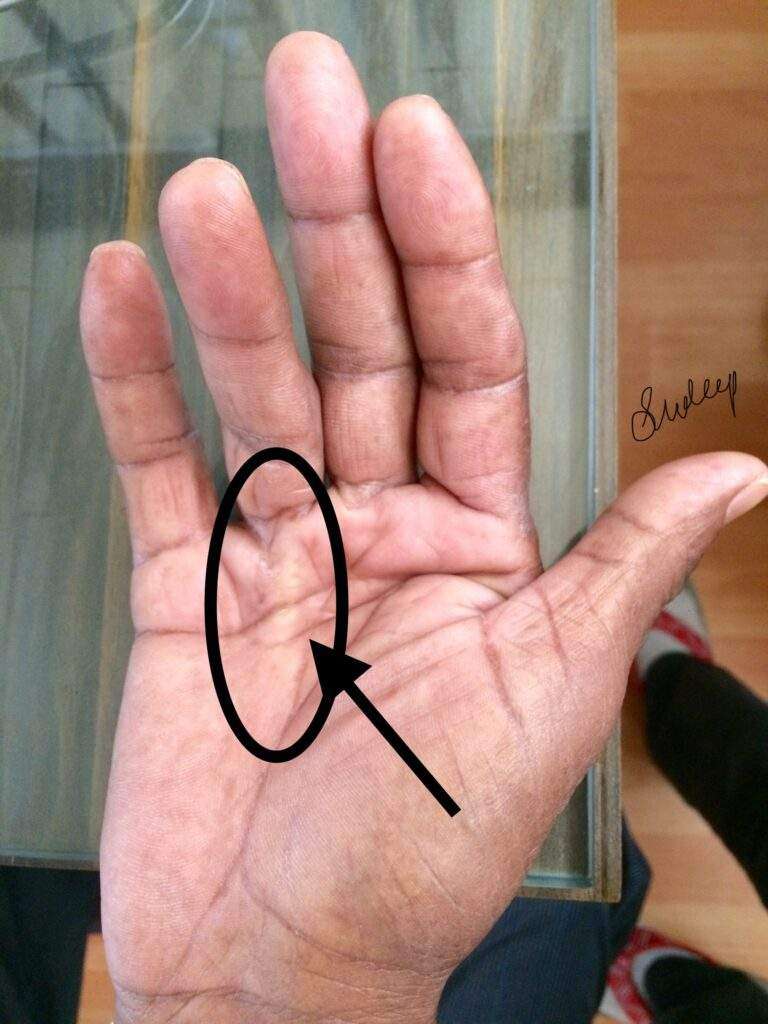
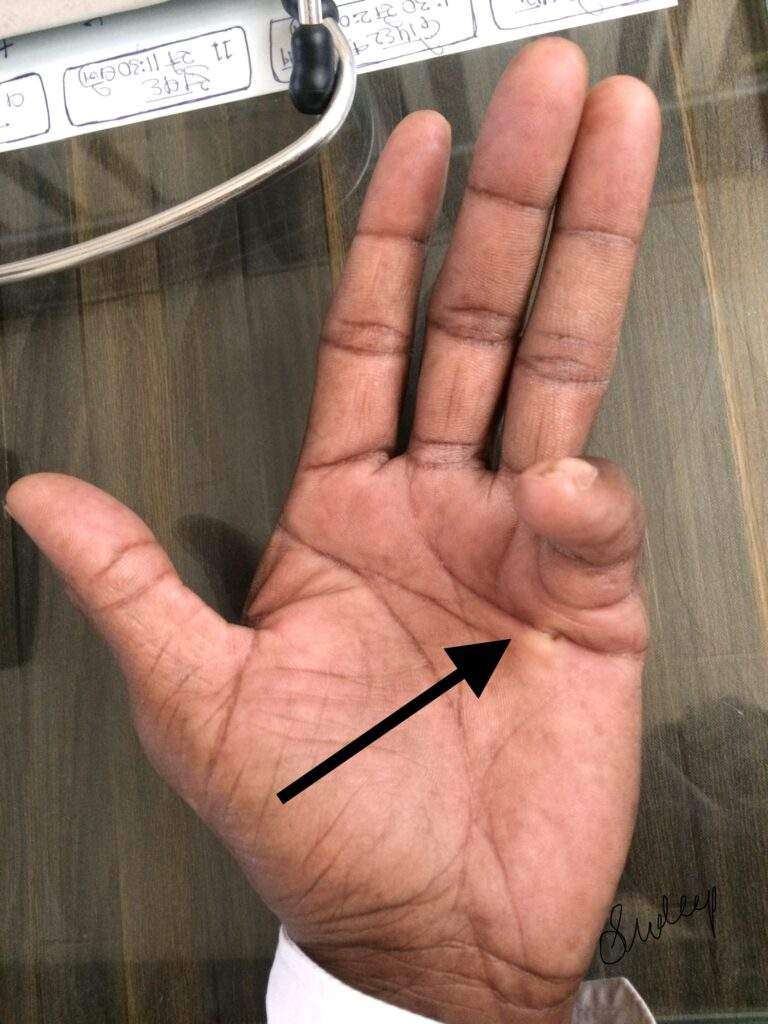
Dupuytrens (du-pwe-TRANZ) contracture is a hand deformity that usually develops over years. The condition affects a layer of tissue that lies under the skin of your palm. Knots of tissue form under the skin — eventually creating a thick cord that can pull one or more fingers into a bent position.
The affected fingers can’t be straightened completely, which can complicate everyday activities such as placing your hands in your pockets, putting on gloves or shaking hands.
Dupuytrens contracture mainly affects the two fingers farthest from the thumb, and occurs most often in older men of Northern European descent. A number of treatments are available to slow the progression of Dupuytrens contracture and relieve symptoms.
Symptoms
Dupuytrens contracture typically progresses slowly, over years. The condition usually begins as a thickening of the skin on the palm of your hand. As it progresses, the skin on your palm might appear puckered or dimpled. A firm lump of tissue can form on your palm. This lump might be sensitive to the touch but usually isn’t painful.
In later stages of Dupuytrens contracture, cords of tissue form under the skin on your palm and can extend up to your fingers. As these cords tighten, your fingers might be pulled toward your palm, sometimes severely.
The two fingers farthest from the thumb are most commonly affected, though the middle finger also can be involved. Only rarely are the thumb and index finger affected. Dupuytrens contracture can occur in both hands, though one hand is usually affected more severely.
Causes
Doctors don’t know what causes Dupuytrens contracture. There’s no evidence that hand injuries or occupations that involve vibrations to the hands cause the condition.
Risk factors
A number of factors are believed to increase your risk of the disease, including:
Age. Dupuytrens contracture occurs most commonly after the age of 50.
Sex. Men are more likely to develop Dupuytrens and to have more severe contractures than are women.
Ancestry. People of Northern European descent are at higher risk of the disease.
Family history. Dupuytrens contracture often runs in families.
Tobacco and alcohol use. Smoking is associated with an increased risk of Dupuytrens contracture, perhaps because of microscopic changes within blood vessels caused by smoking. Alcohol intake also is associated with Dupuytrens.
Diabetes. People with diabetes are reported to have an increased risk of Dupuytrens contracture.
Complications
Dupuytren’s contracture can make it difficult to perform certain functions using your hand. Since the thumb and index finger aren’t usually affected, many people don’t have much inconvenience or disability with fine motor activities such as writing. But as Dupuytrens contracture progresses, it can limit your ability to fully open your hand, grasp large objects or to get your hand into narrow places.
Diagnosis
In most cases, doctors can diagnose Dupuytrens contracture by the look and feel of your hands. Other tests are rarely necessary.
Your doctor will compare your hands to each other and check for puckering on the skin of your palms. He or she will also press on parts of your hands and fingers to check for toughened knots or bands of tissue.
Your doctor also might check to see if you can put your hand flat on a tabletop or other flat surface. Not being able to fully flatten your fingers indicates you have Dupuytrens contracture.
Treatment
If the disease progresses slowly, causes no pain and has little impact on your ability to use your hands for everyday tasks, you might not need treatment. Instead, you can wait and see if Dupuytrens contracture progresses. You may wish to follow the progression with a tabletop test, which you can do on your own.
Treatment involves removing or breaking apart the cords that are pulling your fingers toward your palm. This can be done in several ways. The choice of procedure depends on the severity of your symptoms and other health problems you may have.
Needling
This technique uses a needle, inserted through your skin, to puncture and break the cord of tissue that’s contracting a finger. Contractures often recur but the procedure can be repeated.
The main advantages of the needling technique are that there is no incision, it can be done on several fingers at the same time, and usually very little physical therapy is needed afterward. The main disadvantage is that it can’t be used in some places in the finger because it could damage a nerve or tendon.
Enzyme injections
Injecting a type of enzyme into the taut cord in your palm can soften and weaken it — allowing your doctor to later manipulate your hand in an attempt to break the cord and straighten your fingers. The FDA has approved collagenase Clostridium histolyticum for this purpose. The advantages and disadvantages of the enzyme injection are similar to needling. Enzyme injections are not offered at all medical institutions.
Surgery
Another option for people with advanced disease, limited function and progressing disease is to surgically remove the tissue in your palm affected by the disease. The main advantage to surgery is that it results in a more complete and longer-lasting release than that provided by the needle or enzyme methods. The main disadvantages are that physical therapy is usually needed after surgery, and recovery can take longer.
In some severe cases, especially if surgery has failed to correct the problem, surgeons remove all the tissue likely to be affected by Dupuytren’s contracture, including the attached skin. In these cases a skin graft is needed to cover the open wound. This surgery is the most invasive option and has the longest recovery time. People usually require months of intensive physical therapy afterward.
Lifestyle and home remedies
If you have mild Dupuytrens contracture, you can protect your hands by:
Avoiding a tight grip on tools by building up the handles with pipe insulation or cushion tape
Using gloves with heavy padding during heavy grasping tasks
However, your condition may persist or worsen, despite these precautions.
Preparing for your appointment
While you might first bring your symptoms to the attention of your family doctor, he or she might refer you to a specialist doctor.
What you can do
Before your appointment, you might want to write a list that answers the following questions:
Do you have a family history of this problem?
What treatments have you tried? Did they help?
What medications and supplements do you take regularly?
Blood clots are lifesavers when they seal a cut. They can be dangerous, even deadly, when they form inside an artery or vein. Deep vein thrombosis (sometimes called DVT) is the formation of a blood clot in a large leg vein. It can also occur in an arm vein. Deep vein thrombosis can lead to a pulmonary embolism, or sometimes a stroke.
Blood that circulates to the legs and feet must flow against gravity on its journey back to the heart. The trip is aided by the contraction of leg muscles during walking or fidgeting. The contractions squeeze veins, pushing blood through them. Small flaps, or valves, inside the veins keep blood flowing in the direction of the heart.
Anything that slows blood flow through the arms and legs can set the stage for a blood clot to form. This can range from having an arm or leg immobilized in a cast to prolonged sitting or being confined to bed. Things that make blood more likely to clot, such as genetic disorders and cancer, are other triggers for deep-vein thrombosis.
Symptoms of deep vein thrombosis and pulmonary embolism
Deep vein thrombosis can develop silently. It can also cause:
pain or tenderness in a leg or arm that gets worse with time, not better
swelling in one leg or arm
a reddish or bluish tinge to the skin of one leg or arm
a leg or arm that feels warm to the touch.
The symptoms of pulmonary embolism include:
difficulty breathing
chest pain or discomfort that worsens with a deep breath or cough
coughing up blood
a fast heart rate
sudden lightheadedness or fainting
Diagnosing deep vein thrombosis and pulmonary embolism
To diagnose DVT, your doctor will examine your legs to check for swelling and tenderness. He or she will ask about your symptoms and risk factors.
Based on the findings, your doctor may order a D-Dimer blood test or an ultrasound of your legs.
The blood test measures the level of a chemical called D-Dimer. It is almost always abnormally high when blood clots are actively forming in the body.
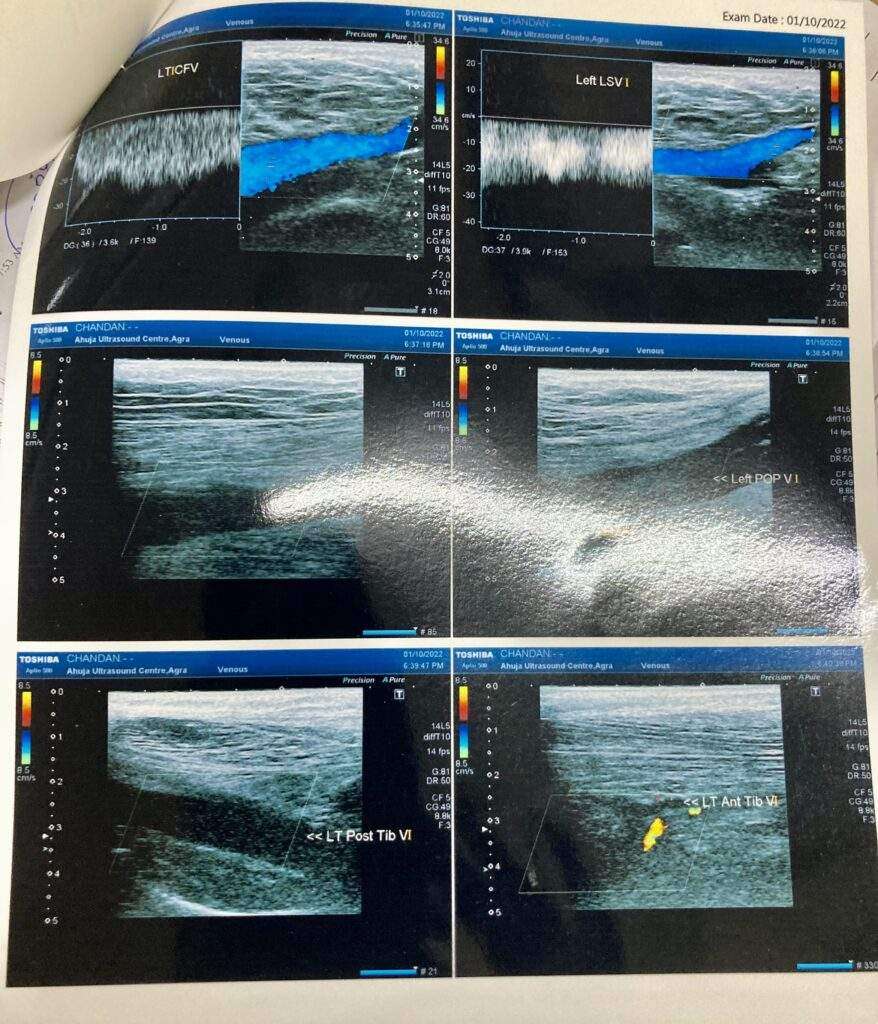
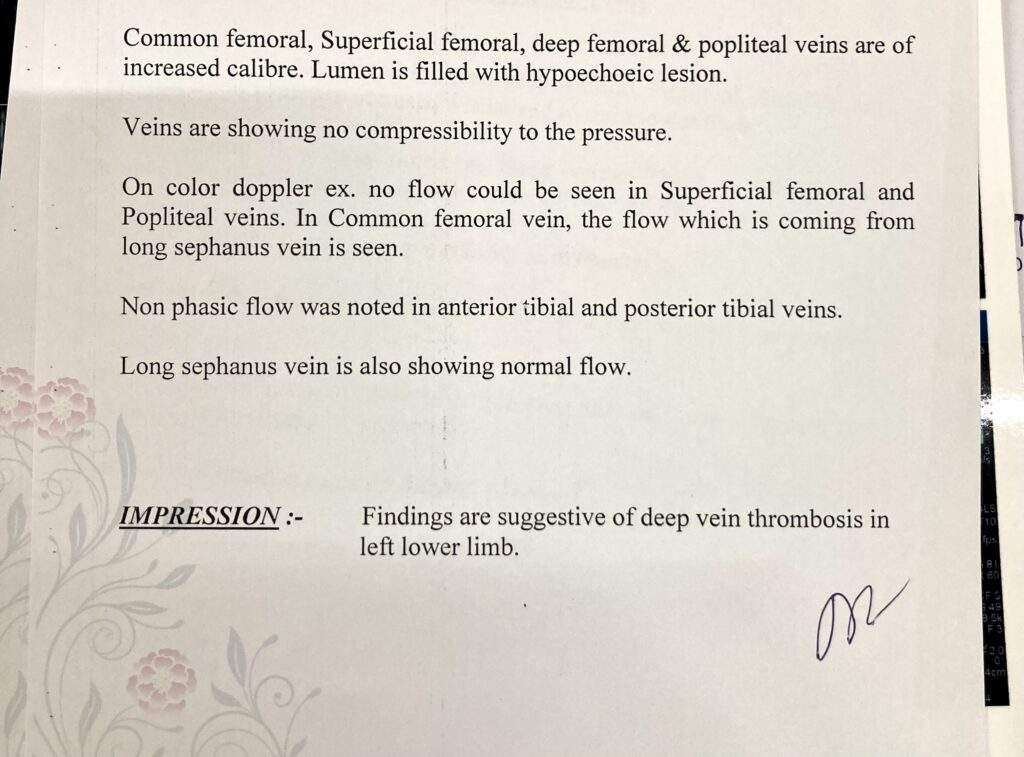
An ultrasound of your legs is done to look for blood flow problems in your veins. This procedure is called a lower extremity non-invasive test, or LENI. If the LENI shows evidence of a blood clot, your doctor will diagnose DVT.
If the initial LENI is negative, it does not mean that there is no clot. It may be too early to see the full effect of the clot. Your doctor may ask that you return in three to four days for a repeat LENI.
If your doctor suspects you have a pulmonary embolism, he or she will first try to determine if you have DVT. If the LENI shows one or more blood clots in your leg veins, and you have symptoms of a pulmonary embolism, an embolism is the most likely diagnosis.
Or your doctor may order computed tomography (CT) of the chest. The test requires an IV injection of dye to look for blood clots in the pulmonary arteries. People that have impaired kidney function or an allergy to the dye might need a different type of lung scan called a V/Q scan to examine lung blood flow.
Treating deep vein thrombosis
The initial treatment for a DVT or pulmonary embolism is heparin or one of the newer oral anti-coagulant drugs. These medications act on certain blood proteins to prevent new blood clot formation and therefore help unwanted clots get smaller. They are commonly called “blood thinners.”
There are two main types of heparin. The oldest type of heparin is best administered by a constant intravenous infusion. Another type of heparin is called low-molecular-weight heparin. It is injected under the skin once or twice per day.
Two of the newer anti-coagulant drugs are approved for initial treatment of DVT and pulmonary embolism: rivaroxaban (Xarelto) and apixaban (Eliquis).
If you have a DVT without a pulmonary embolism, you may not need to be hospitalized. You could be treated at home with injections of a low-molecular-weight heparin or either rivaroxaban or apixaban.
Some people may need to start therapy in the hospital. In this case, the type of heparin used is determined by many factors. These include body weight, kidney function and other circumstances.
If you have a pulmonary embolism, you will probably be hospitalized. If so, you likely will be treated with either type of heparin initially. But oral rivaroxaban or apixaban could be an option instead of heparin if your pulmonary embolism is small.
If you are started on either IV heparin or low-molecular weight heparin shots under the skin, your doctor will transition you to an oral drug. Traditional oral therapy has been warfarin (Coumadin). For decades, it was the only oral drug to treat DVT and pulmonary embolism.
In addition to rivaroxaban and apixaban, two other oral anti-coagulant drugs can be used after heparin: dabigatran (Pradaxa) and edoxapan (Savaysa). More of these types of drugs will be approved soon.
Warfarin takes a few days to start working. Once a blood test shows that warfarin is effective, you will stop taking heparin. You will continue taking warfarin for several months or longer.
During the first few weeks that you take warfarin, you will continue to need frequent blood tests to make sure you are taking the right amount. Once your blood test results consistently show that you are taking the right amount of medication, blood can be drawn every two to four weeks.
Some foods—especially green, leafy vegetables that contain large amounts of vitamin K—can alter the blood-thinning action of warfarin. Ask your doctor or pharmacist for a list of these foods. You can continue to eat these foods as long as you eat approximately the same amount of them each day. That way, the effect on your medication will be consistent.
Other medications can also affect how warfarin works in your body. Tell any doctor who is prescribing medications for you that you are taking warfarin.
The new novel oral anti-coagulants don’t require regular blood testing. They are given in a fixed dose. The other advantage is not worrying about eating food with too much vitamin K.